
Chapter 7 – Breast
Palpable Breast Mass
ACR – Palpable Breast Mass
Case
Palpable Breast Mass
Clinical:
History: This 51 year old, female, patient discovered a left breast lump while in the shower. It was not present on her last physical examination one year ago. She had a family history of breast cancer in her maternal grandmother and her maternal aunt.
Symptoms: She felt a lump in the left breast above the nipple.
Signs: No evidence of skin thickening or nipple retraction. A hard, but slightly mobile, tumor was felt with lobulated margins. No lymph nodes palpable.
DDx:
Variant of anatomy
Benign breast tumor – cyst, fibroadenoma, fibrocystic change, fat necrosis, radial scar, abscess.
Malignant breast tumor
Metastatic disease to the breast
Imaging Recommendation
Palpable breast mass, Woman 40 year of age, or older, initial evaluation, Variant 1.
Mammography
The evaluation of a palpable abnormality most often begins with mammography and/or breast tomosynthesis. Imaging analysis of the lesion features will lead to a recommendation for further management based upon the ACR, Breast Imaging Reporting and Data System (BI-RADS).
If mammography is suspicious for malignancy the next examination would usually be an ultrasound of the mass and the ipsilateral axilla.
Breast/Axillary Ultrasound
Imaging Assessment
Findings:
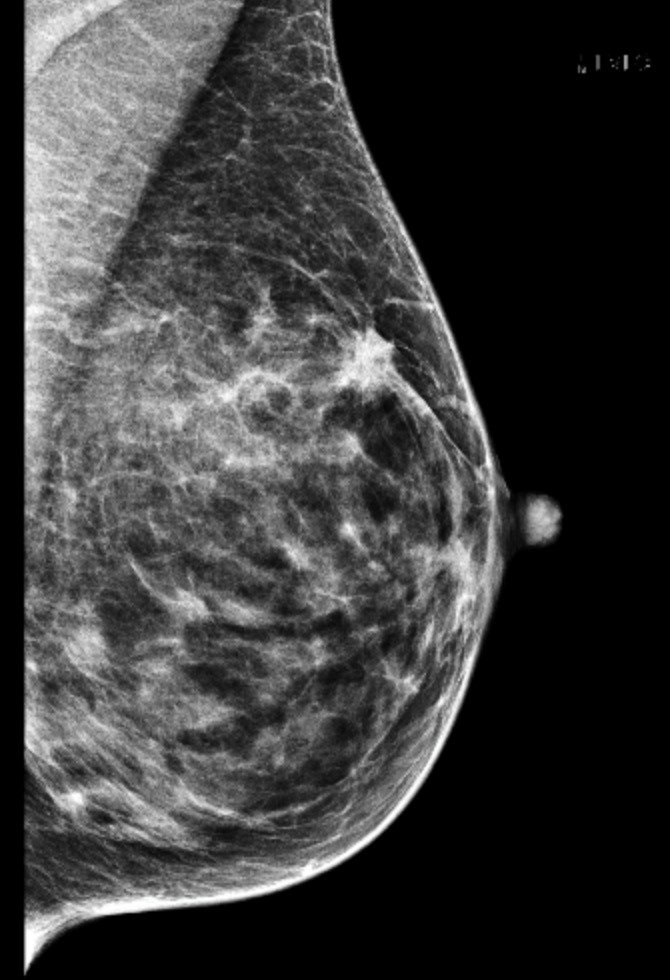
Left Mammography
There was a 1.5 – 2 cm lobulated, spiculated, mass, with minimal architectural distortion, in the left breast at the 2 o’clock location roughly 2.5 – 3 cm cranial to the nipple. The mass does not efface with targeted, focal compression, imaging. Ultrasound of the breast was recommended. No skin abnormalities identified.
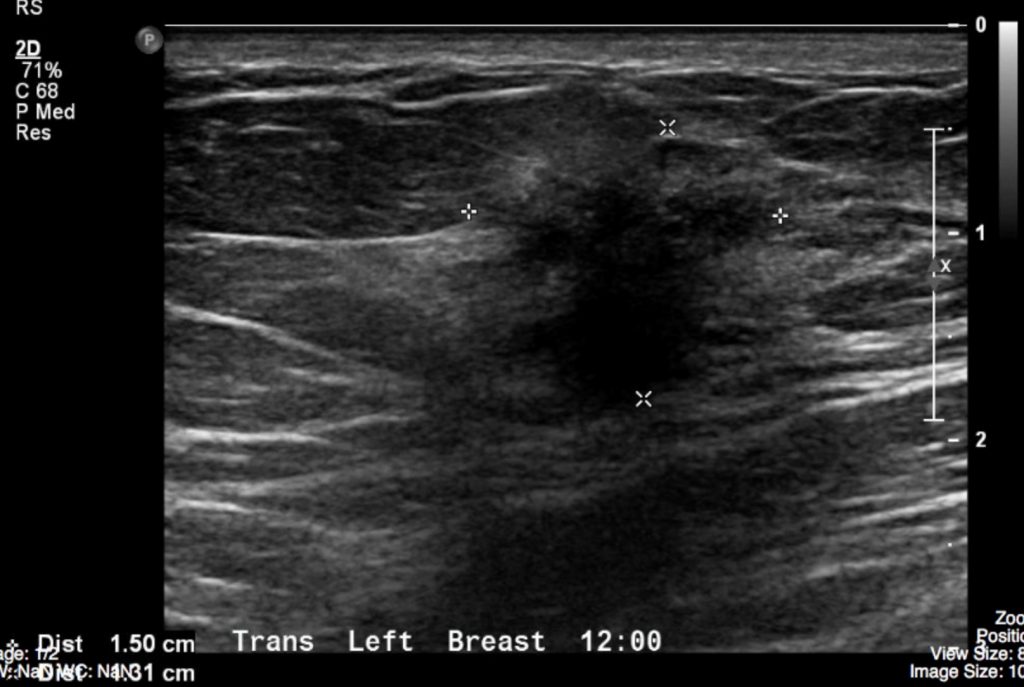
Left Breast Ultrasound
A lobulated, spiculated, mass was detected 2 cm from the nipple at the 2 o’clock location. It was taller than wide and demonstrated acoustic shadowing. No satellite lesions seen. The left axillary images were normal.
Interpretation:
The mass in the left breast had malignant features on mammography and breast ultrasound.
BI-RADS 5, high suspicion for malignancy, tissue diagnosis was recommended.
Diagnosis:
Breast mass with malignant features
Pathology:
Ultrasound Guided Core Biopsy of the mass was performed.
Invasive Ductal Carcinoma was diagnosed on microscopic assessment.
Discussion:
Breast cancer is the most common female malignancy and the second leading cause of female cancer death. Between 20,000 – 25,000 new cases of breast cancer will be diagnosed in Canada a year. Most palpable breast lumps are benign, but a new palpable breast mass is a common presenting sign of breast cancer. These masses may be detected by patient self-examination or during a physical examination carried out by a health professional.
Mammographic findings may include:
- Atypical breast calcification(s)
- Visible soft tissue mass(es)
- Tissue architectural distortion
- Skin thickening
- Skin retraction
- Nipple retraction
- Asymmetry in breast size
Attributions
Figure 7.5A Mammography image of a breast mass by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC-BY-NC-SA 4.0 license.
Figure 7.5B Ultrasound image of a breast mass by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC-BY-NC-SA 4.0 license.
