
Case Studies
Case 1. Chloe
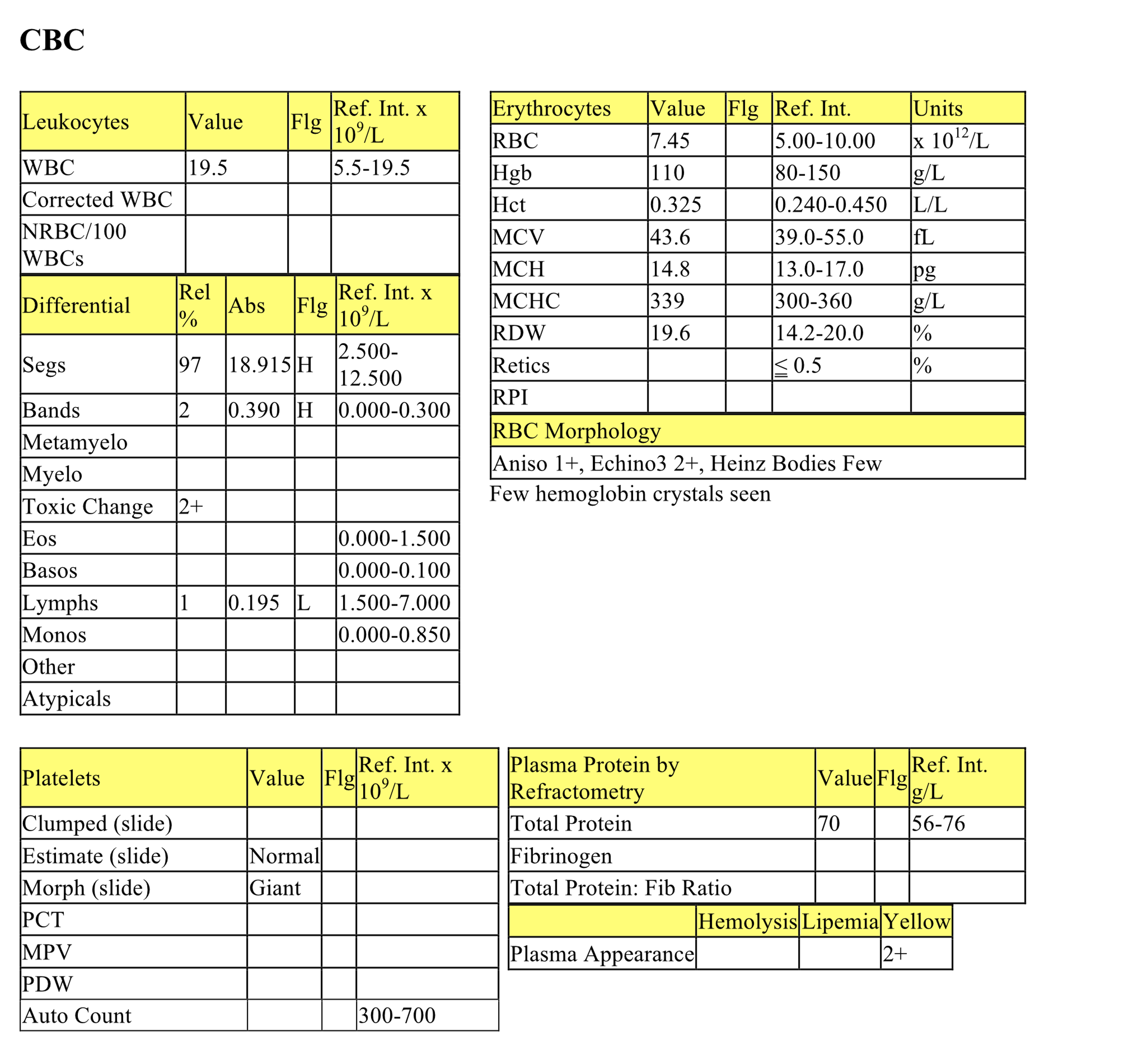
Chloe, a 2 year old FS DSH cat, had lethargy and inappetence for 1 week. Physical findings included iritis, icterus, and excess abdominal fluid.
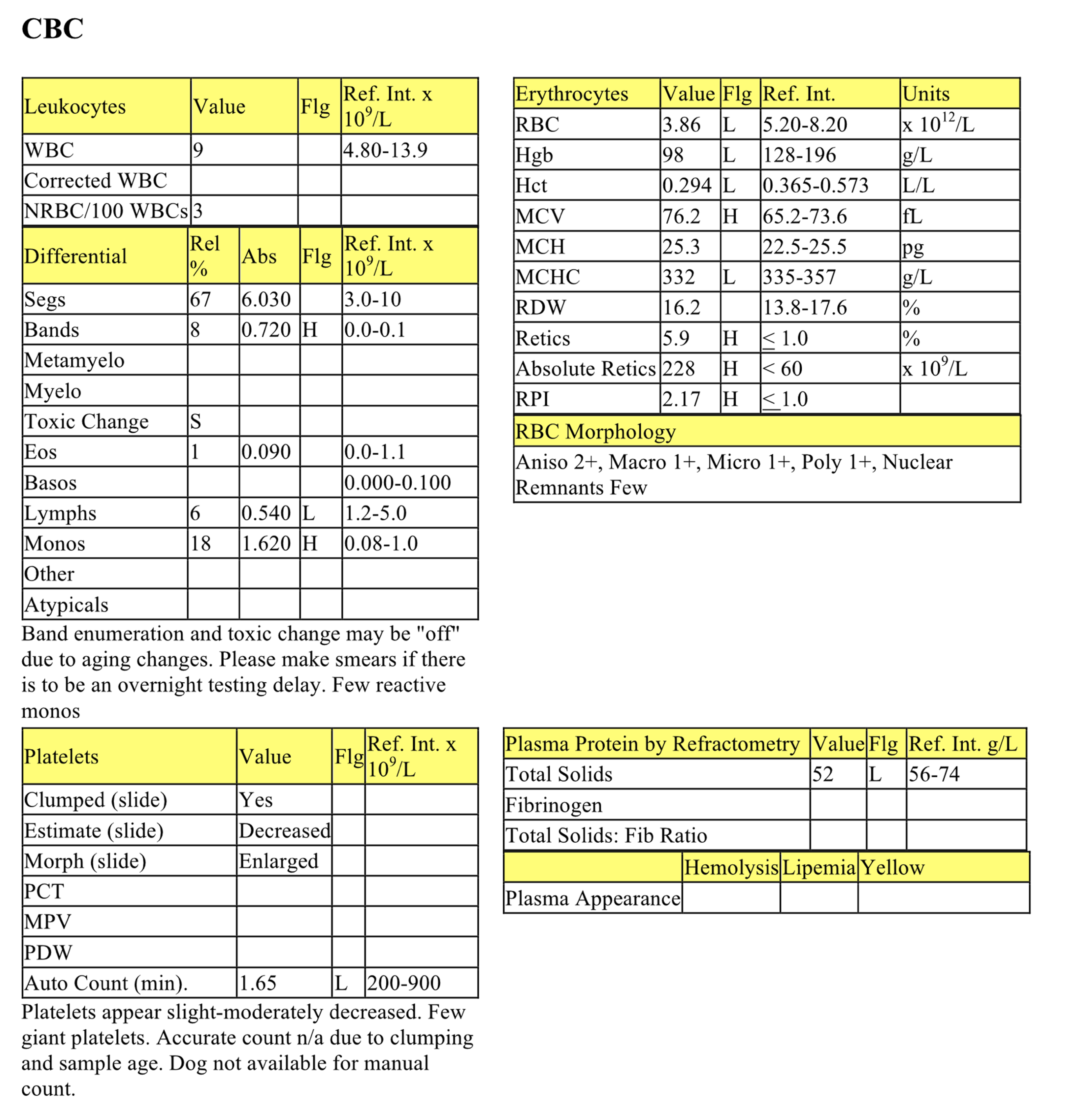
CBC
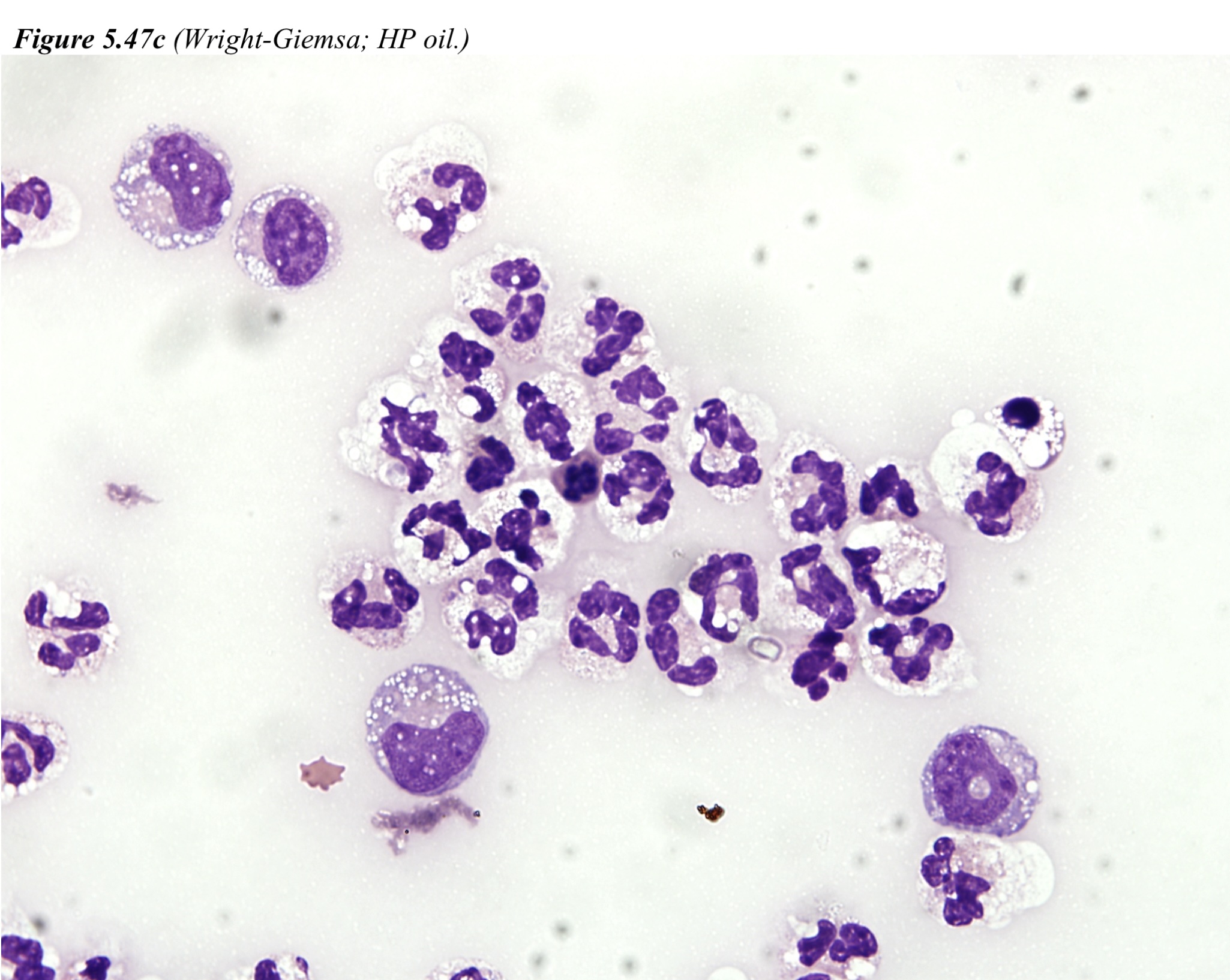
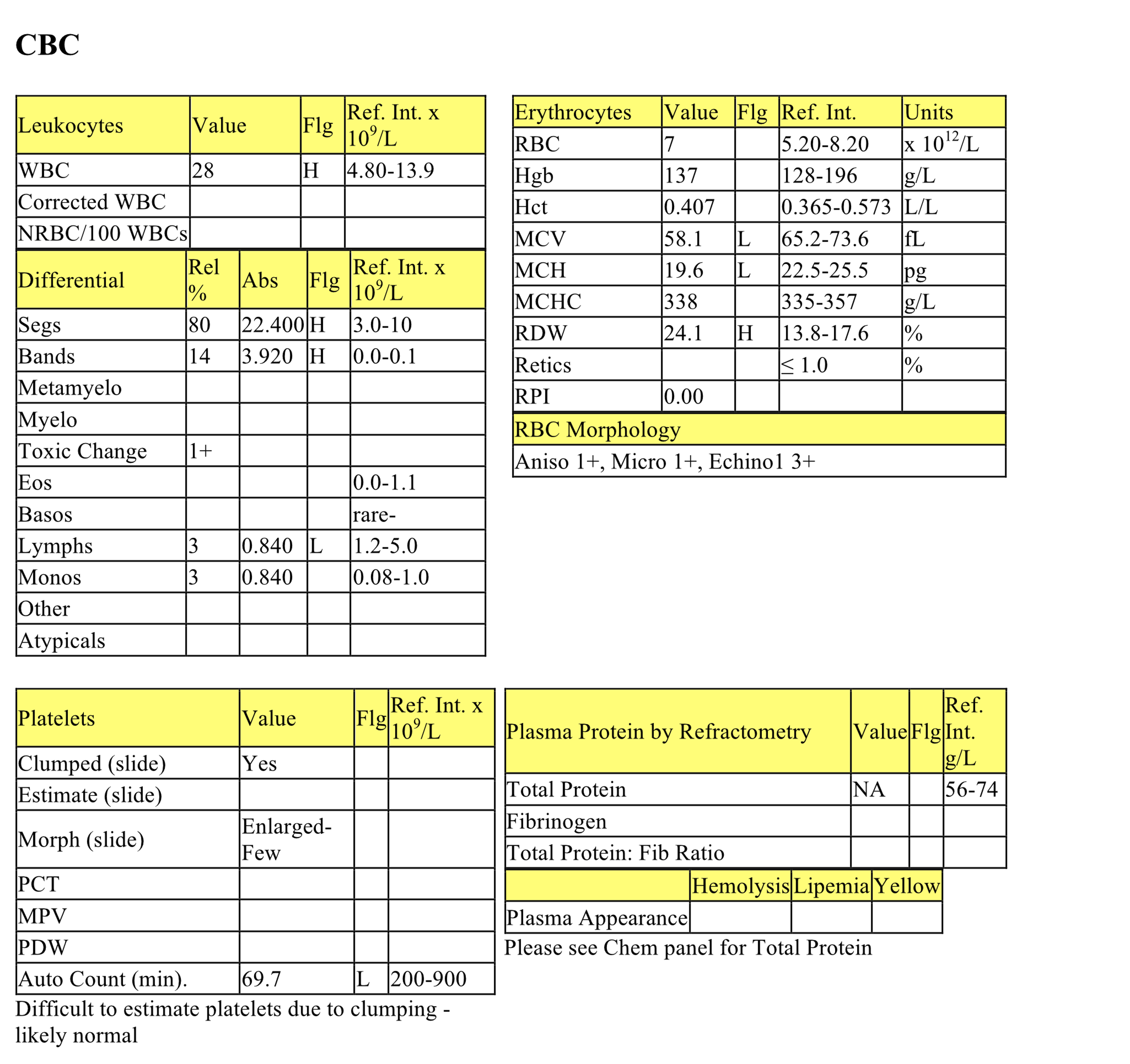
The erythrogram is unremarkable; hemoglobin crystallization sometimes occurs in vitro. Echinocytes III could also be an in vitro change since electrolyte and acid-base abnormalities are not detected on the biochemical panel. Few Heinz bodies can be normal in the cat. Leukocytes are high normal and there is a mild to moderate neutrophilia with a mild left shift, moderate toxic change, and severe lymphopenia. These findings indicate inflammation and stress. The plasma is yellow and this is explained by icterus.
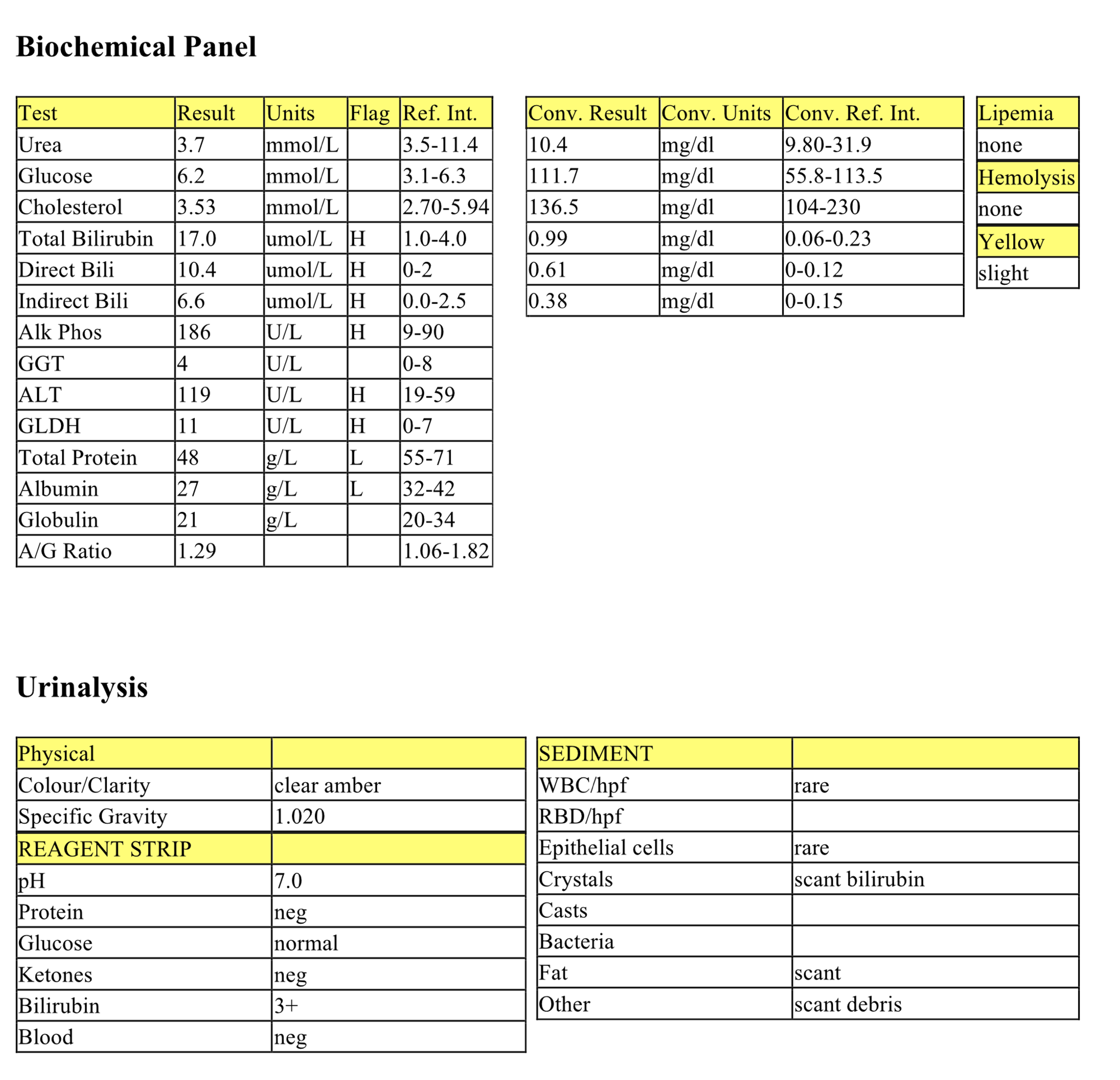
Biochemical Panel
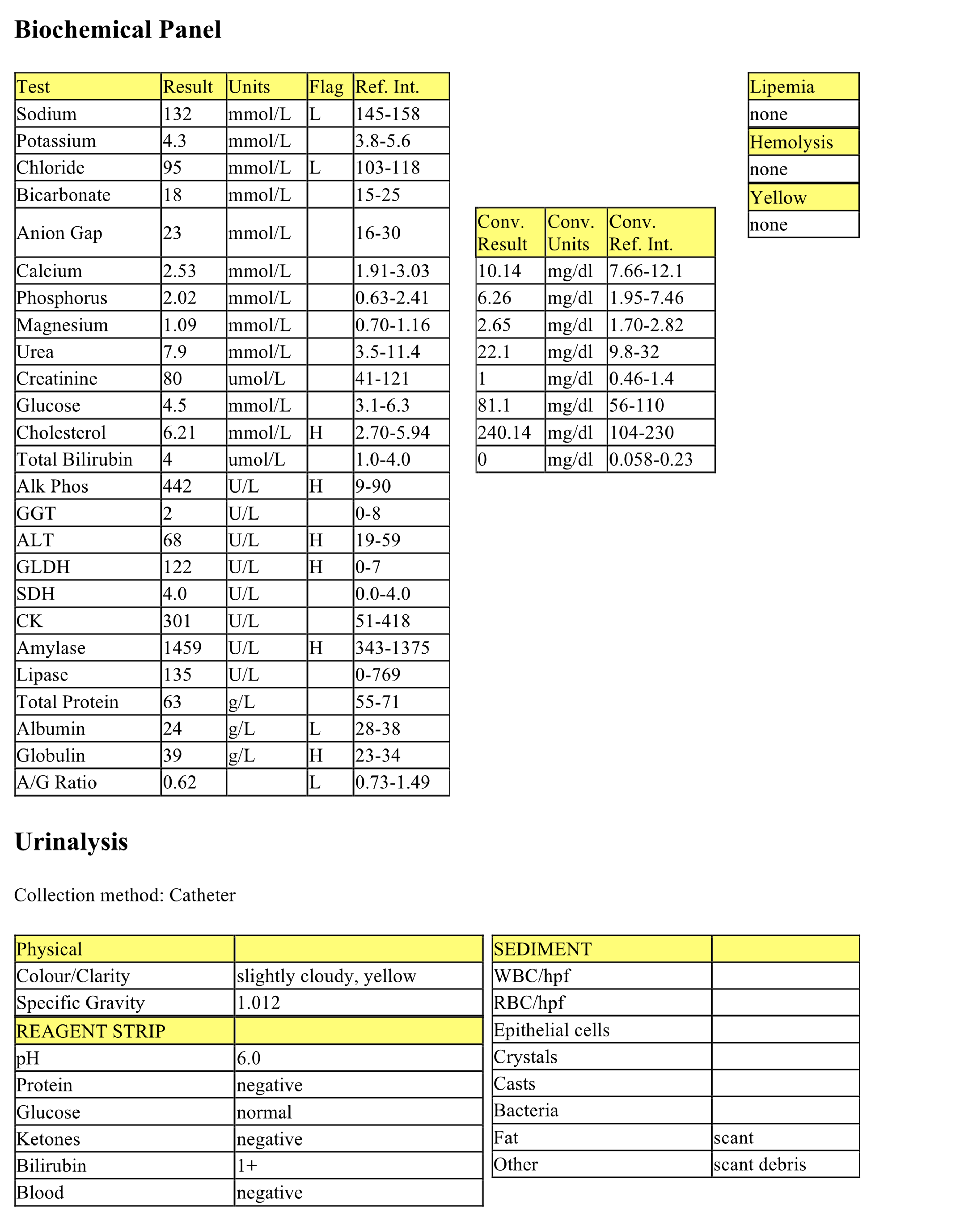
Many changes are mild and may not be clinically significant. Mild hyponatremia and hypochloremia are likely not significant, but could reflect decreased intake given the history of inappetence. Mild hypocalcemia relates to hypoalbuminemia. The mild hyperphosphatemia is not associated with azotemia and may not be significant. Decreased creatinine is likely not significant but could reflect decreased muscle mass. Mild hyperglycemia may be due to stress. Hyperbilirubinemia and increased ALP activity are best explained by cholestasis. Mild hyperamylasemia is likely not significant. Hypoalbuminemia, hyperglobulinemia, and low albumin to globulin ratio may be due to decreased albumin synthesis as a negative acute phase protein and increased globulin synthesis from increased acute phase proteins, increased gammaglobulins from antigenic stimulation, or both. Protein loss into the abdominal cavity should be considered, but is expected to result in a panhypoproteinemia.
Abdominal Fluid
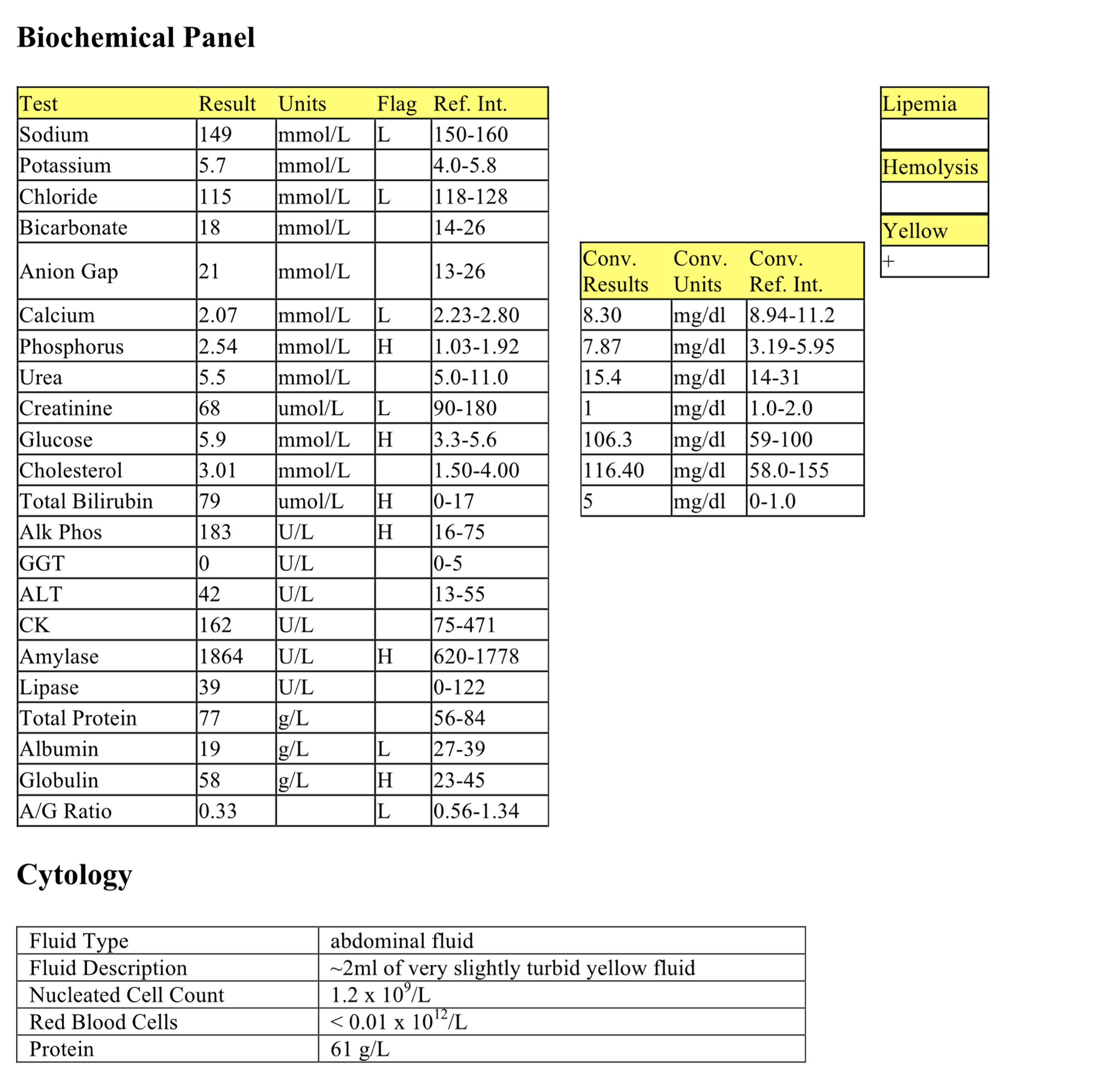
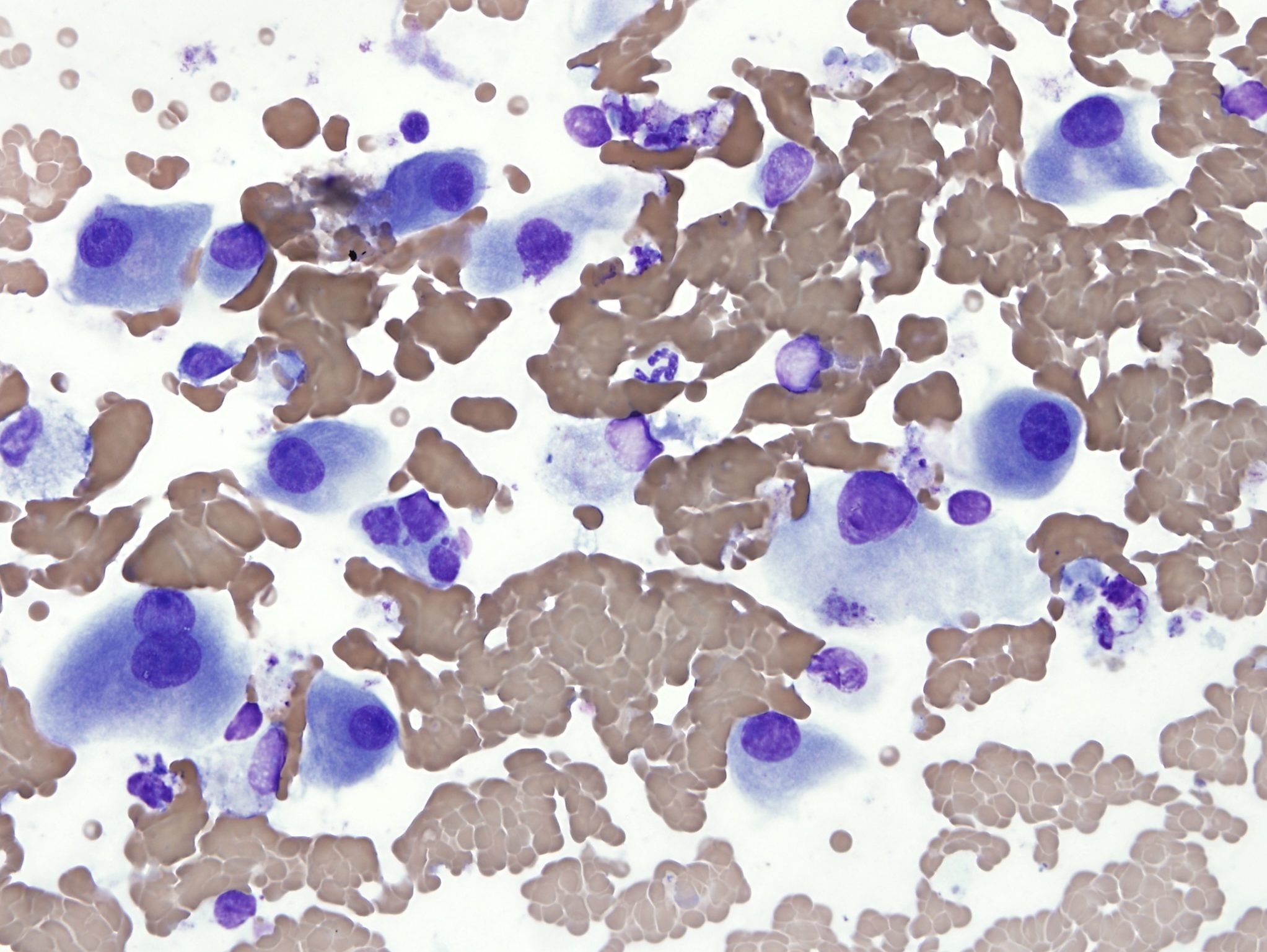
The nucleated cell count and protein concentration of the abdominal fluid meet the criteria of a modified transudate. However, a protein concentration of this magnitude is highly suggestive of feline infectious peritonitis (FIP) virus infection which causes fluid exudation due to vasculitis, an inflammatory process. The heavily stippled appearance of the background on the direct smear is from the high protein content of the fluid. Although the nucleated cells are low in number, they comprise a mixed population of inflammatory cells, also suggestive of FIP (see also Fig. 5.38). Note that Fig. 5.47b is a cytospin sample, which has been diluted, thus the protein stippling in the background is no longer present.
- Chloe did have FIP, which causes vasculitis and mixed neutrophilic and macrophagic inflammation. Hepatic involvement is frequent, as are effusions into body cavities. Such effusions have variable nucleated cell counts, but typically have very high protein content. Serum protein electrophoresis usually demonstrates a polyclonal gammopathy resulting from chronic antigenic stimulation. Unfortunately, this humoral response to the virus is ineffective. History, clinical and laboratory findings often provide sufficient information to diagnose FIP. Immunohistochemistry to detect viral antigen in tissues can confirm the diagnosis.
Case 2. Tundra
Tundra, a 10 year old Mc Siberian Husky dog, had lethargy, anorexia, and pale mucous membranes.
CBC
Tundra’s hematocrit is within the reference interval but microcytes are present on the blood smear, MCV and MCH are mildly decreased, and MCHC is low normal. Microcytosis can occur with iron deficiency, hepatic dysfunction, and occasionally with chronic disease/inflammation. It can also be seen in certain dog breeds, including Siberian Husky dogs, which is the likely reason in this case. There is a moderate leukocytosis characterized by a mild to moderate neutrophilia, significant left shift, mild toxic change, and mild to moderate lymphopenia. The leukogram changes indicate significant inflammation, with an appropriately responsive bone marrow, and stress.
Biochemical Panel
Mild hyponatremia and hypochloremia could be due to loss into the abdomen in this case (see below), coupled with decreased intake. Mild hypercholesterolemia may reflect cholestasis (unlikely to be post prandial given history of anorexia). Mild hyperamylasemia is unlikely to be significant. The mild increase in ALP activity could be from steroid induction if the dog has been sick/stressed for some time. Alternatively, there may be cholestasis, though bilirubin and GGT are not affected. Increases in GLDH activity and ALT activity indicate hepatocellular injury. Hypoalbuminemia, mild hyperglobulinemia, and low albumin to globulin ratio suggest decreased albumin synthesis (as a negative acute phase protein), and increased globulin synthesis from increased acute phase proteins, increased gammaglobulin synthesis from antigenic stimulation, or both.
Urinalysis
The urine is not concentrated, but without azotemia or dehydration, this may not be significant. 1+ bilirubin can be normal in canine urine.
Abdominal Fluid
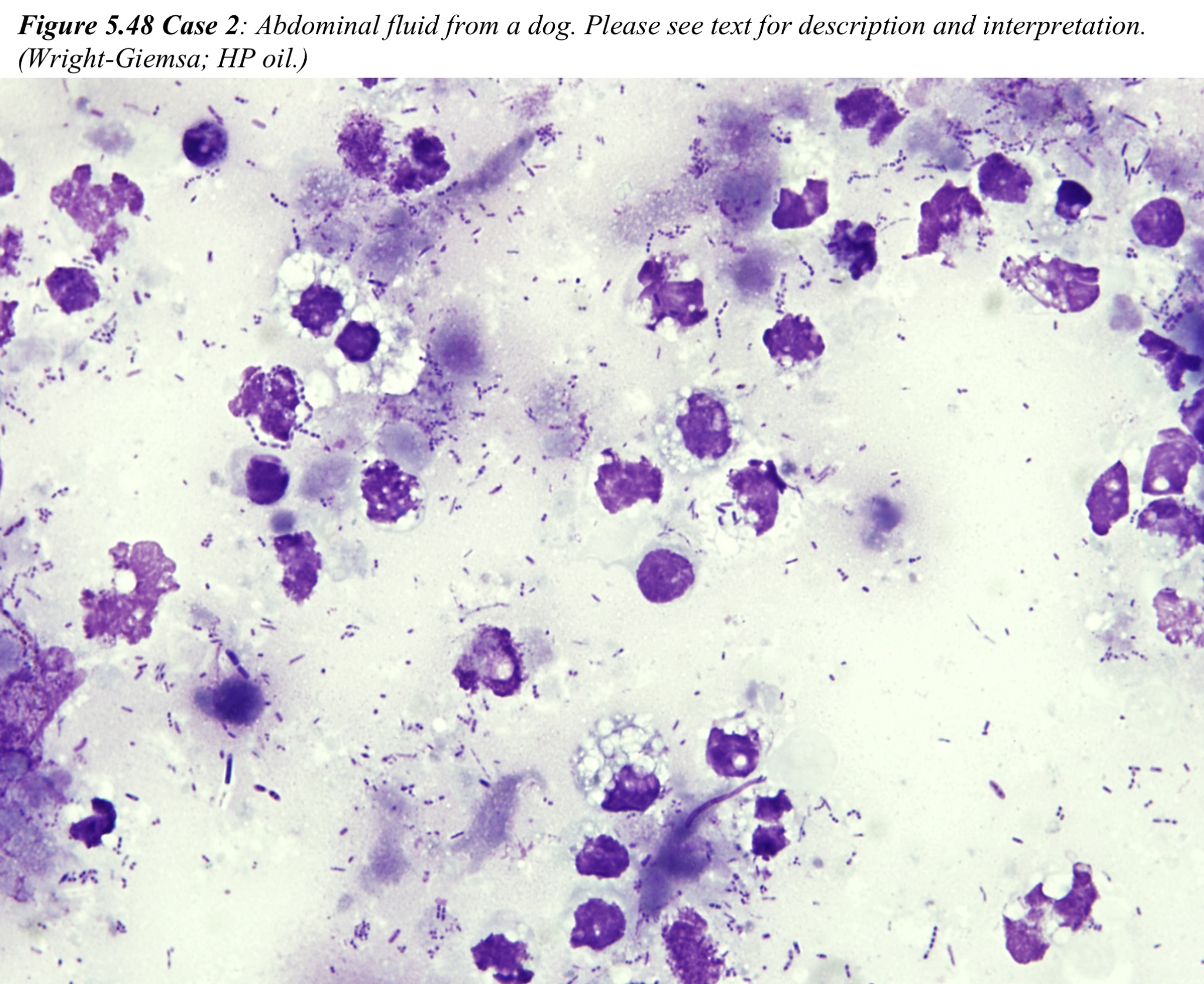
The nucleated cell count and protein content are high – this fluid is an exudate. Degenerate and nondegenerate neutrophils predominate, followed by lower numbers of macrophages and reactive mesothelial cells. There is a mixed bacterial population which appears both intra- and extracellularly. Erythrophagia is present, reflecting prior/ongoing hemorrhage into the abdomen. This fluid represents septic neutrophilic inflammation.
The origin of the sepsis was not determined and, although surgery was recommended, Tundra was treated conservatively with antibiotics and fluids. He was sent home and there is no further follow-up.
Case 3. Danni
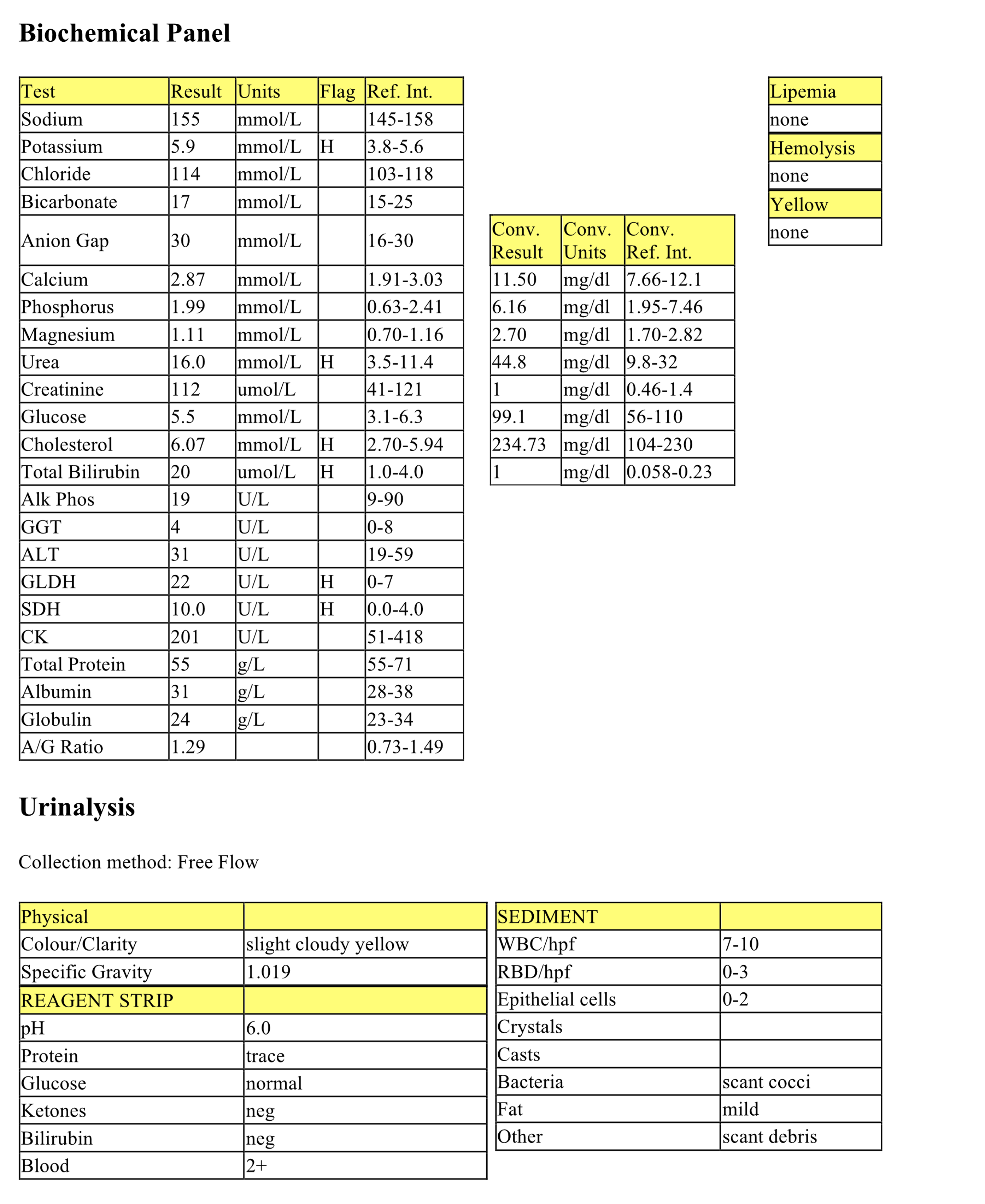
Danni, a 17 year old FS terrier X dog, had excessive weight loss, vomiting, and weakness.
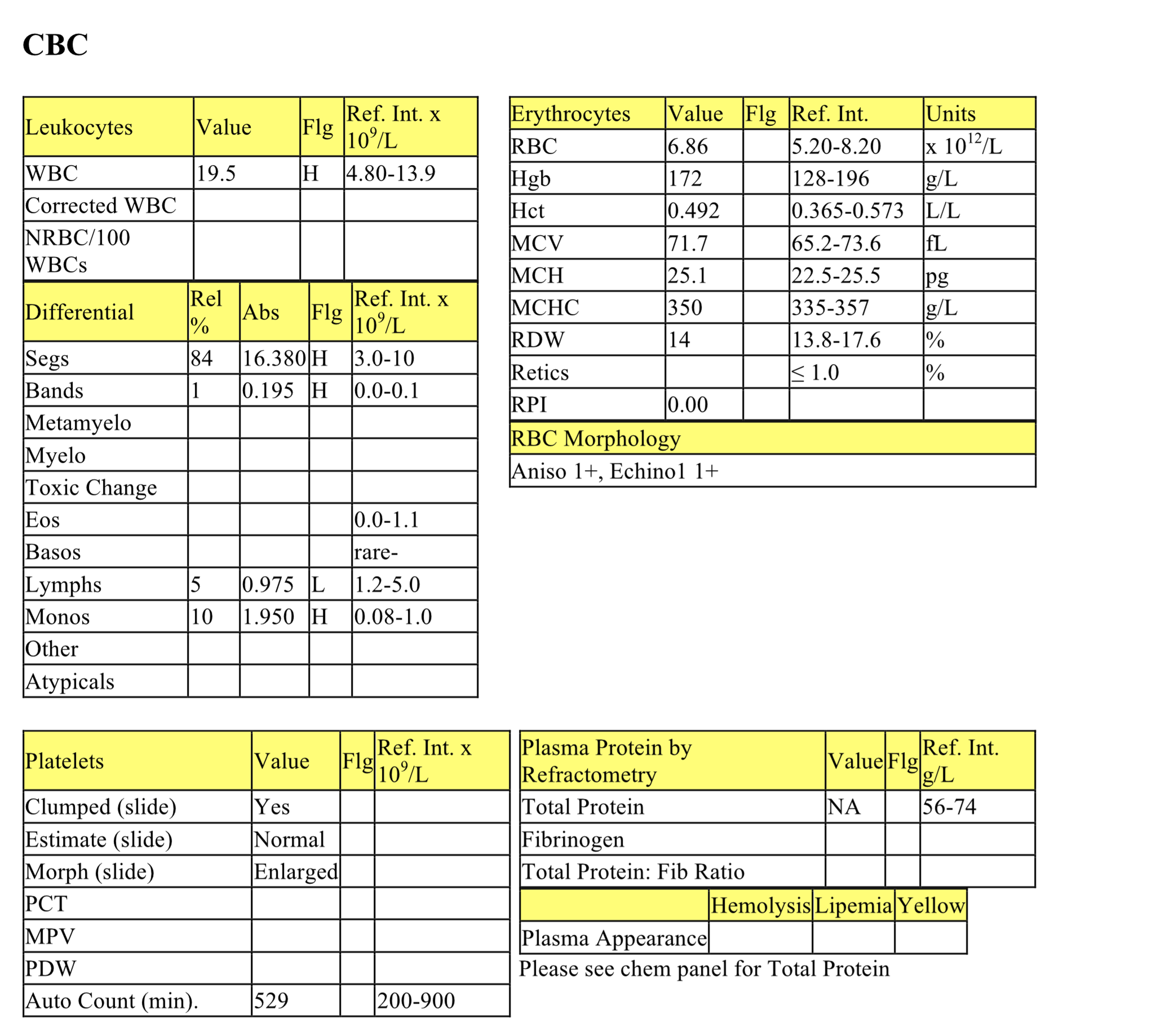
CBC
The CBC is unremarkable except for the leukogram changes which could all be explained by stress; however, concurrent inflammation cannot be ruled out.
Biochemical Panel
Mild hyperkalemia could be due to leakage from leukocytes and platelets since the serum had not been separated from the cells prior to submission to the laboratory; renal retention of potassium is also possible. Mildly increased urea may represent renal azotemia given the urine specific gravity; loss of muscle mass could explain the lack of concurrent creatinine elevation in this case. Very mild hypercholesterolemia may be postprandial or reflect cholestasis. Mild hyperbilirubinemia is likely of hepatic origin since there is no indication of hemolysis or internal hemorrhage to support increased bilirubin production. Increased activities of GLDH and SDH are likely due to mild hepatocellular damage.
Urinalysis
The lack of urine concentration together with the increased urea suggest renal disease. The urine was a free flow sample, therefore, the sediment findings are not necessarily significant and could be contaminants from the lower urogenital tract. Evaluation of a cystocentesis sample should be considered.
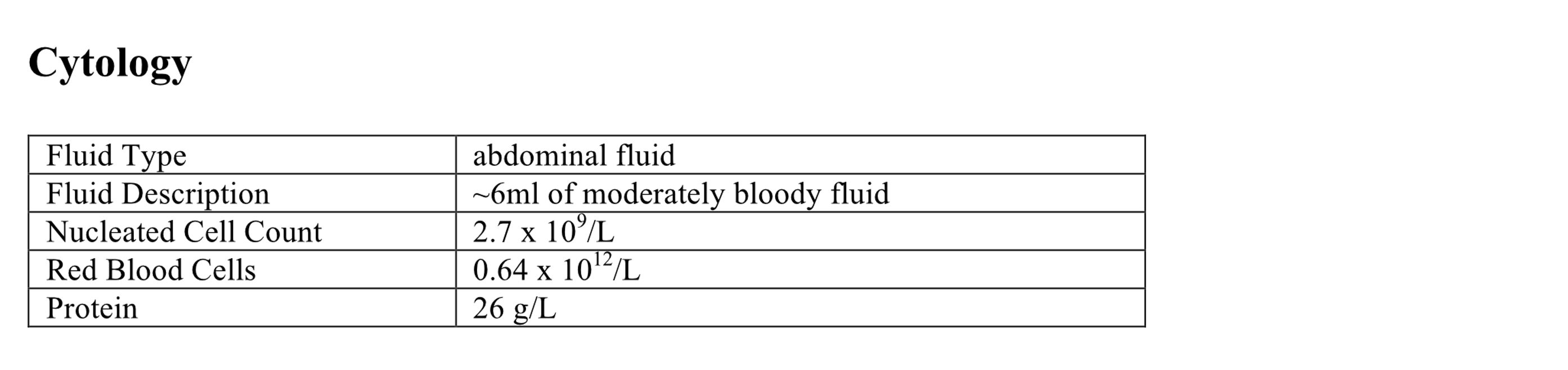
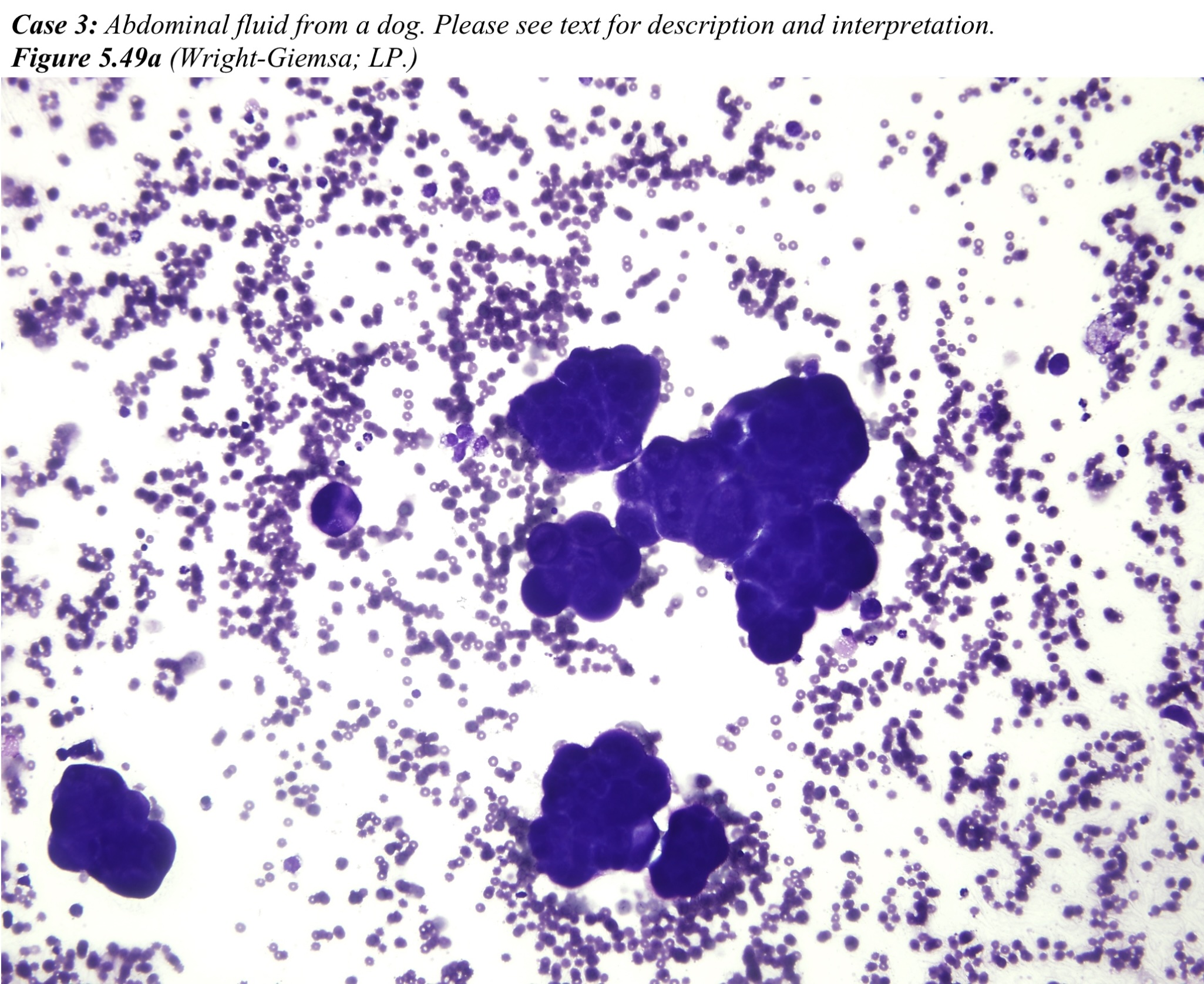
Abdominal Fluid
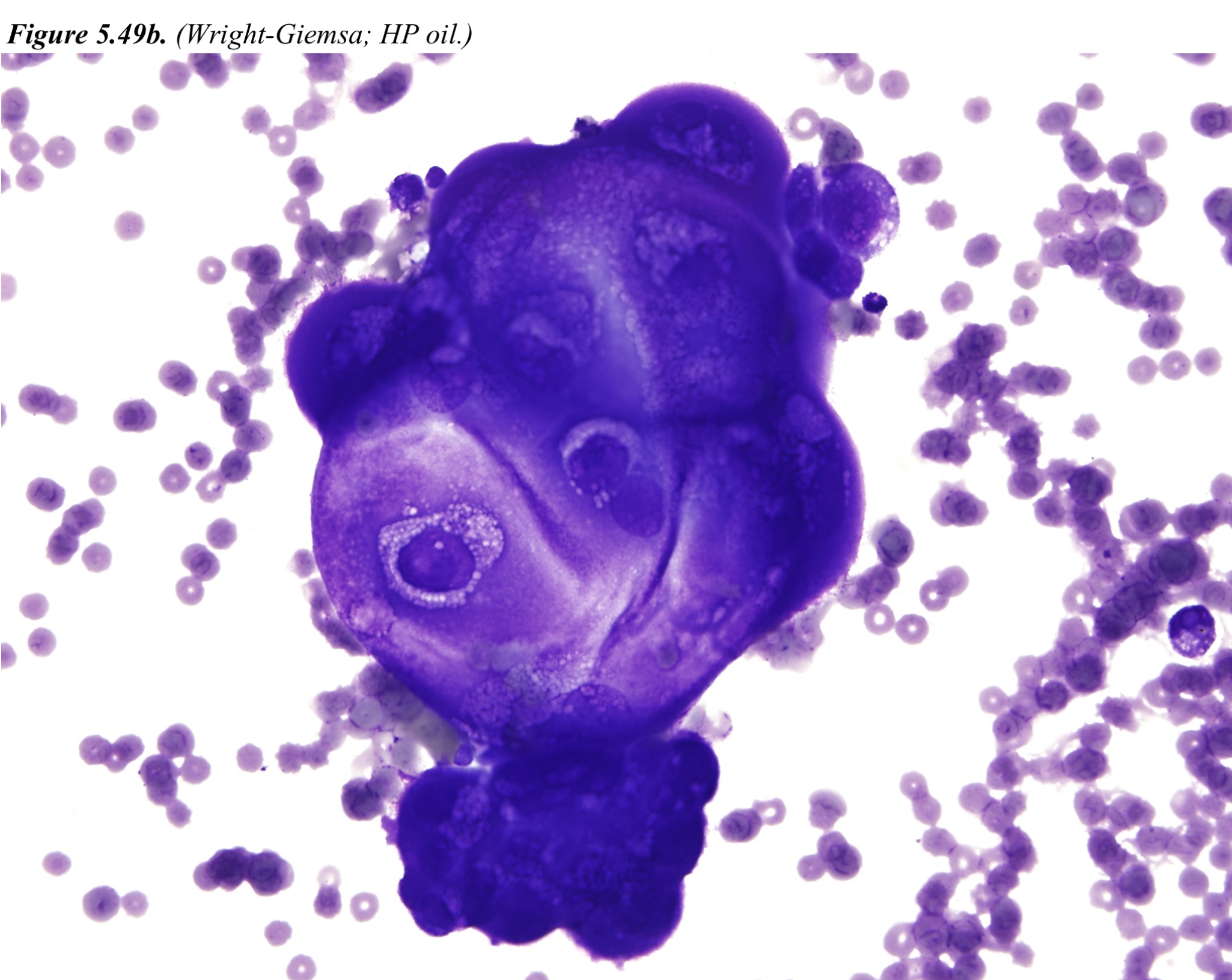
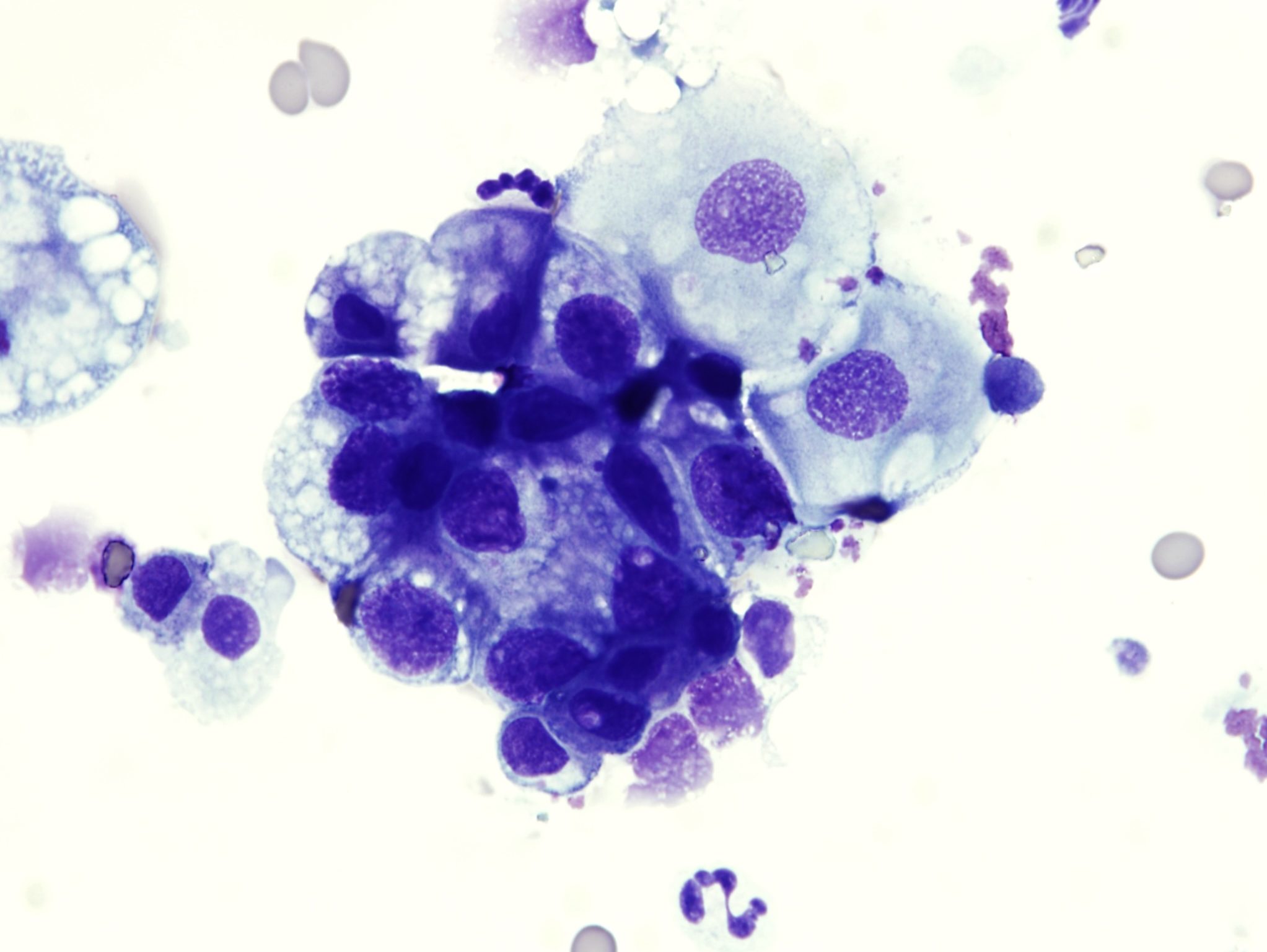
The nucleated cell count and protein content of the fluid are consistent with a modified transudate. Most cells are in large clusters. There is marked anisocytosis and anisokaryosis. Nuclei are oval and basal with coarse chromatin and a single nucleolus. Bi- and trinucleation, with variably sized nuclei, is common. Mitotic figures are occasional. Cytoplasms are darkly stained and sometimes vacuolated. A few macrophages, reactive mesothelial cells, and nondegenerate neutrophils are also present. These findings are consistent with a carcinoma or adenocarcinoma, for example pancreatic or hepatocellular carcinoma, although malignant mesothelioma would also have to be considered.
- Danni was euthanized and a necropsy was not done.
Case 4. Kaleb
Kaleb, a 12 year old M German Shepherd dog, had recent weakness and vomiting. Mucous membranes were pale and there was fluid in the abdomen.
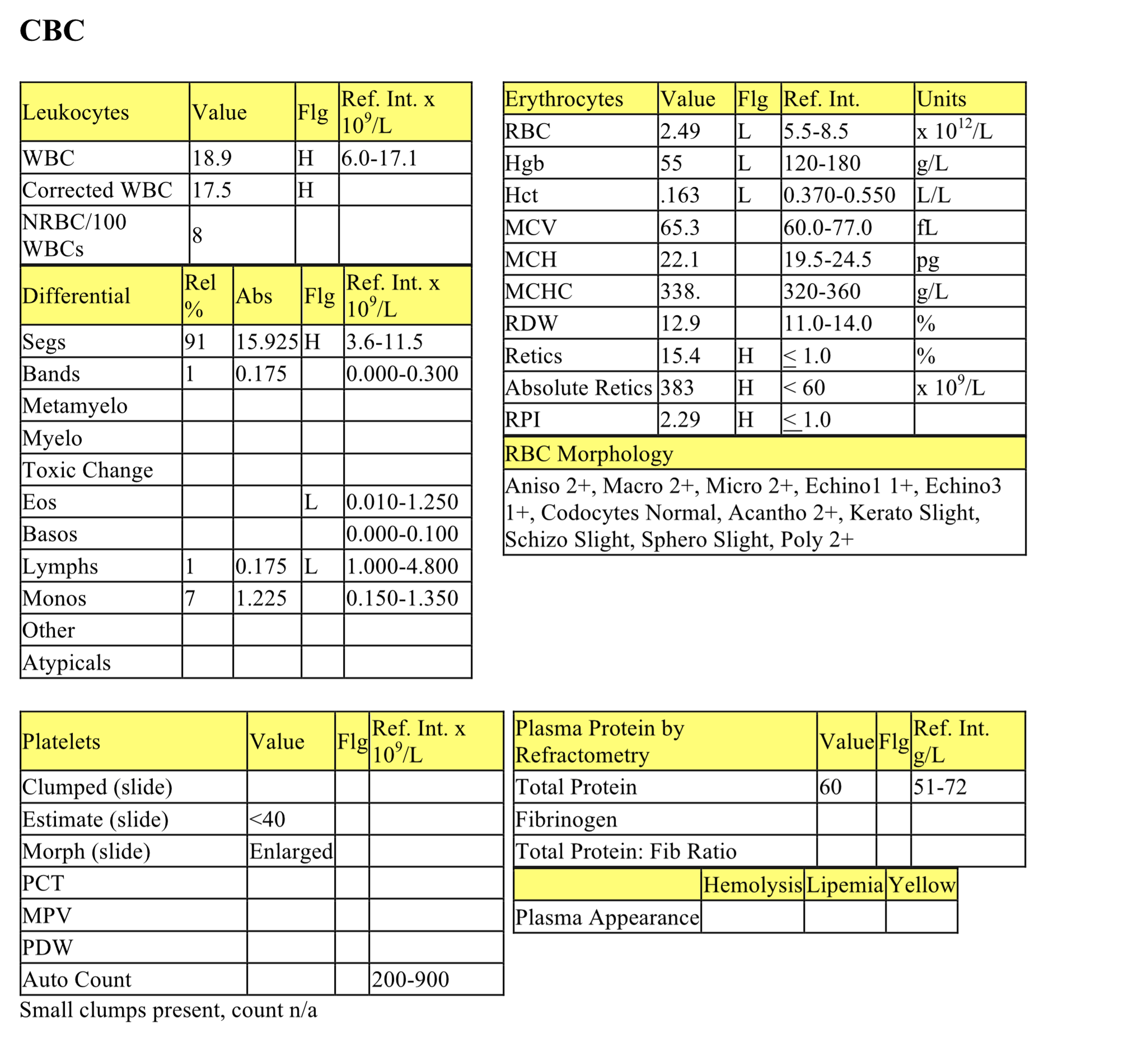
CBC
Kaleb has a marked anemia which is moderately regenerative. Hemorrhage into the abdominal cavity as well as possible disseminated intravascular coagulation and fibrinolysis (DIC&F) could explain the anemia. Acanthocytes are abundant and can be associated with hemangioma or hemangiosarcoma. Keratocytes and schizocytes indicate mechanical shearing of erythrocytes, often due to fibrin strand injury. Leukogram changes are likely due to stress. Platelets are significantly decreased. Keratocytes and schizocytes along with thrombocytopenia suggest possible DIC&F.
Biochemical Panel
Mild hyponatremia and hypochloremia probably represent losses from hemorrhage and vomiting. There is a mild metabolic acidosis with a normal anion gap suggesting bicarbonate loss, which typically occurs through intestinal or renal losses. Mild hyperphosphatemia may reflect decreased renal excretion. Mild azotemia should be interpreted in relation to urine concentrating ability, although prerenal azotemia due to dehydration is likely given the history of vomiting. Decreased lipase is of no pathological significance. Mildly increased ALP activity could be due to cholestasis or enzyme induction from established stress.
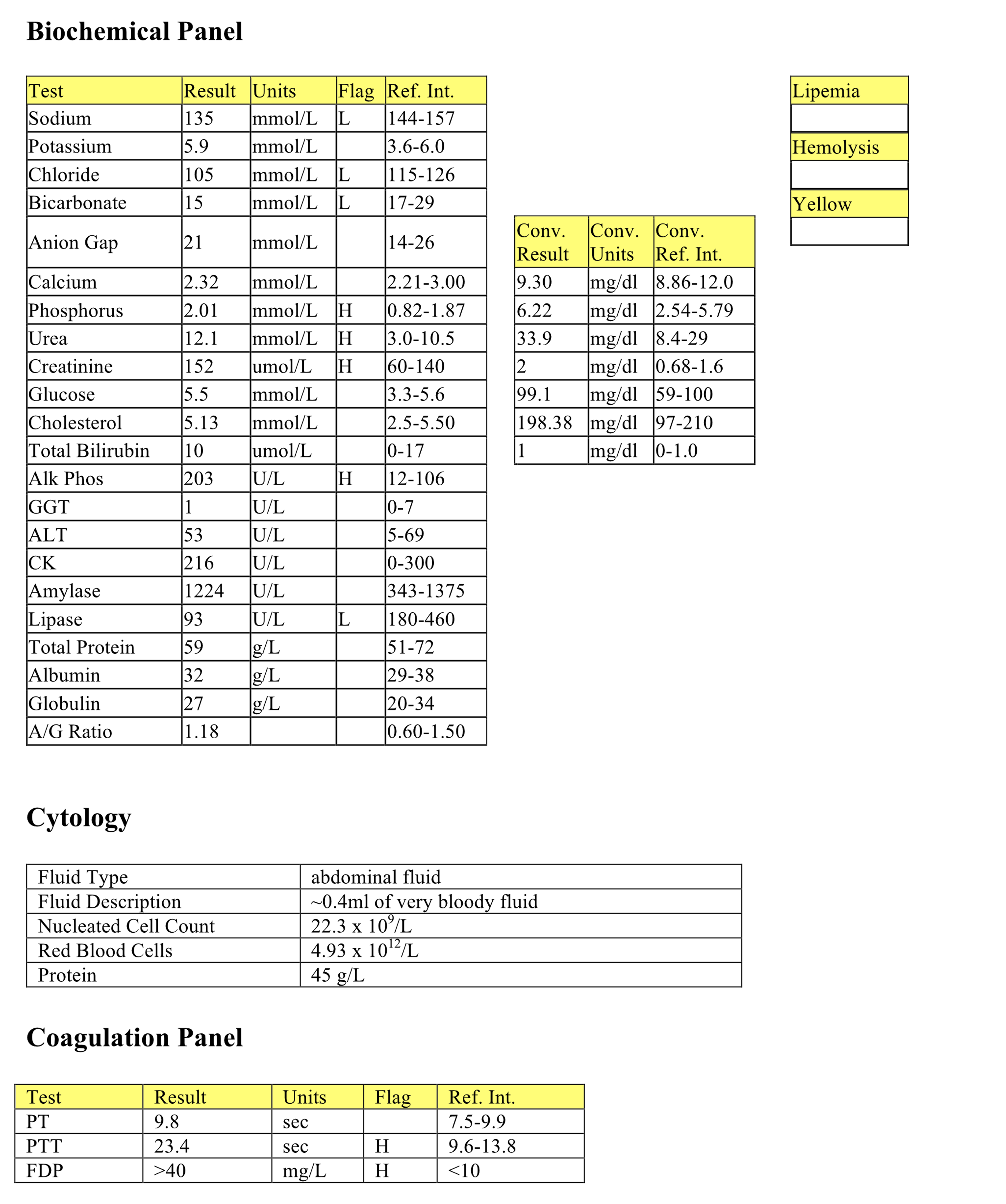
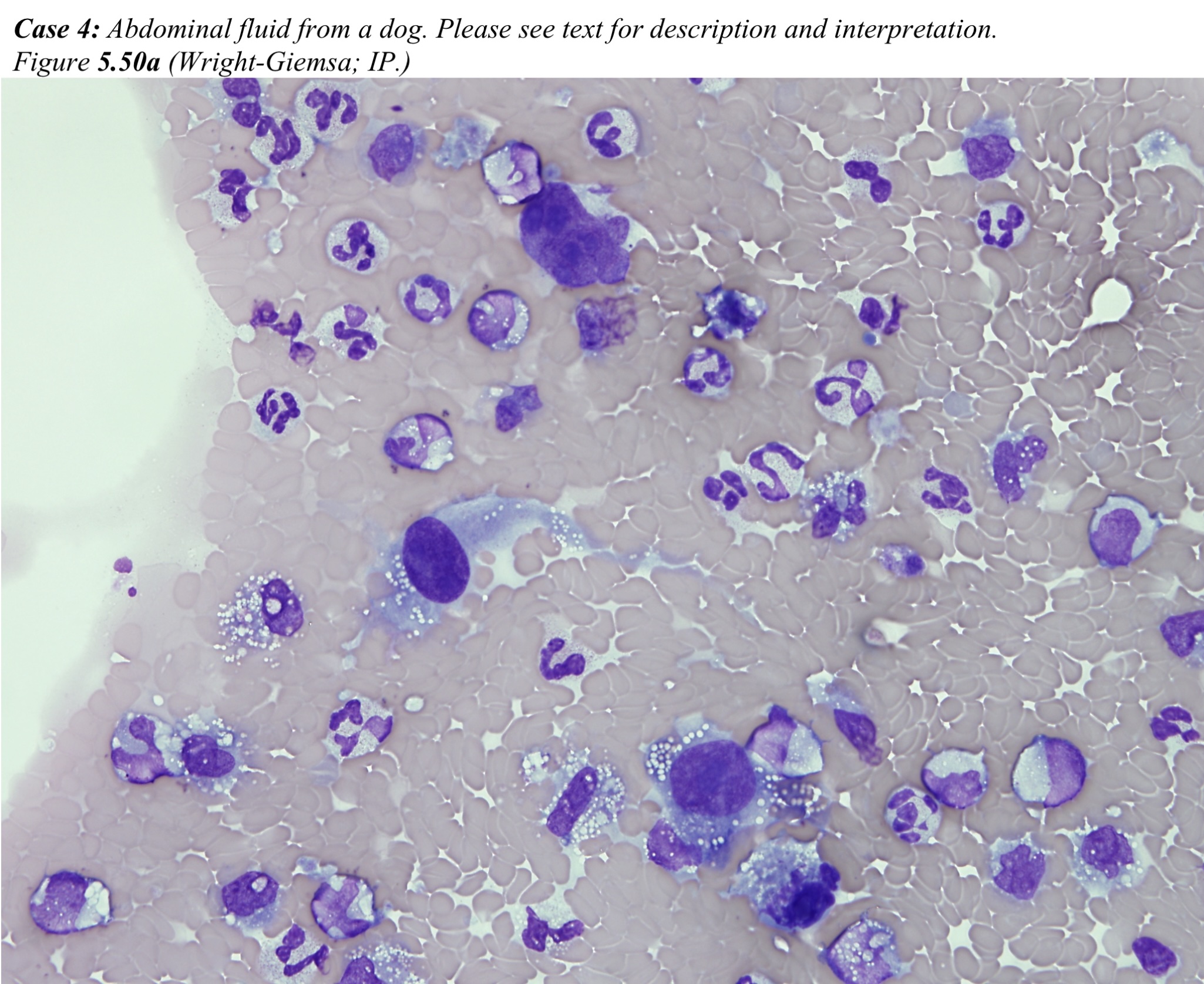
Abdominal Fluid
The fluid represents a hemorrhagic effusion. Numerous free erythrocytes are present. Macrophages, nondegenerate neutrophils, and reactive mesothelial cells predominate, followed by low numbers of eosinophils and lymphocytes. Erythrophagia is commonly seen. Blue-black granular pigment, probably hemosiderin, is present within a few macrophages. Platelets are not present. These cytologic findings indicate both prior and ongoing hemorrhage (see Fig. 5.34). There is also a population of large atypical cells that are spindle to round, with vacuolated cytoplasm and prominent nucleoli.
Coagulation Panel
PTT is prolonged and FDPs are significantly elevated. These findings together with thrombocytopenia and the presence of keratocytes and schizocytes support the presence of DIC&F. PT is often prolonged with DIC&F- in Kaleb it is high normal but it is unclear why it is not prolonged.
- Kaleb’s age and breed, along with the physical and laboratory findings, are highly suggestive of ruptured hemangiosarcoma and subsequent DIC&F. Although splenectomy may be indicated if the tumor is localized to the spleen, Kaleb had evidence of metastasis to other organs in addition to DIC&F, and he was euthanized. Necropsy findings included: hemangiosarcoma involving the right auricle, lung, liver, spleen, and mesentery; hemoperitoneum; and petechial hemorrhages on mucosal and serosal surfaces of the intestines.
Case 5. Ginny
Ginny, an 8 year old Mc DSH cat, had signs of dyspnea for 6 weeks.
CBC
The CBC is unremarkable except for the presence of mild lymphopenia which is probably due to the stress of illness/dyspnea.
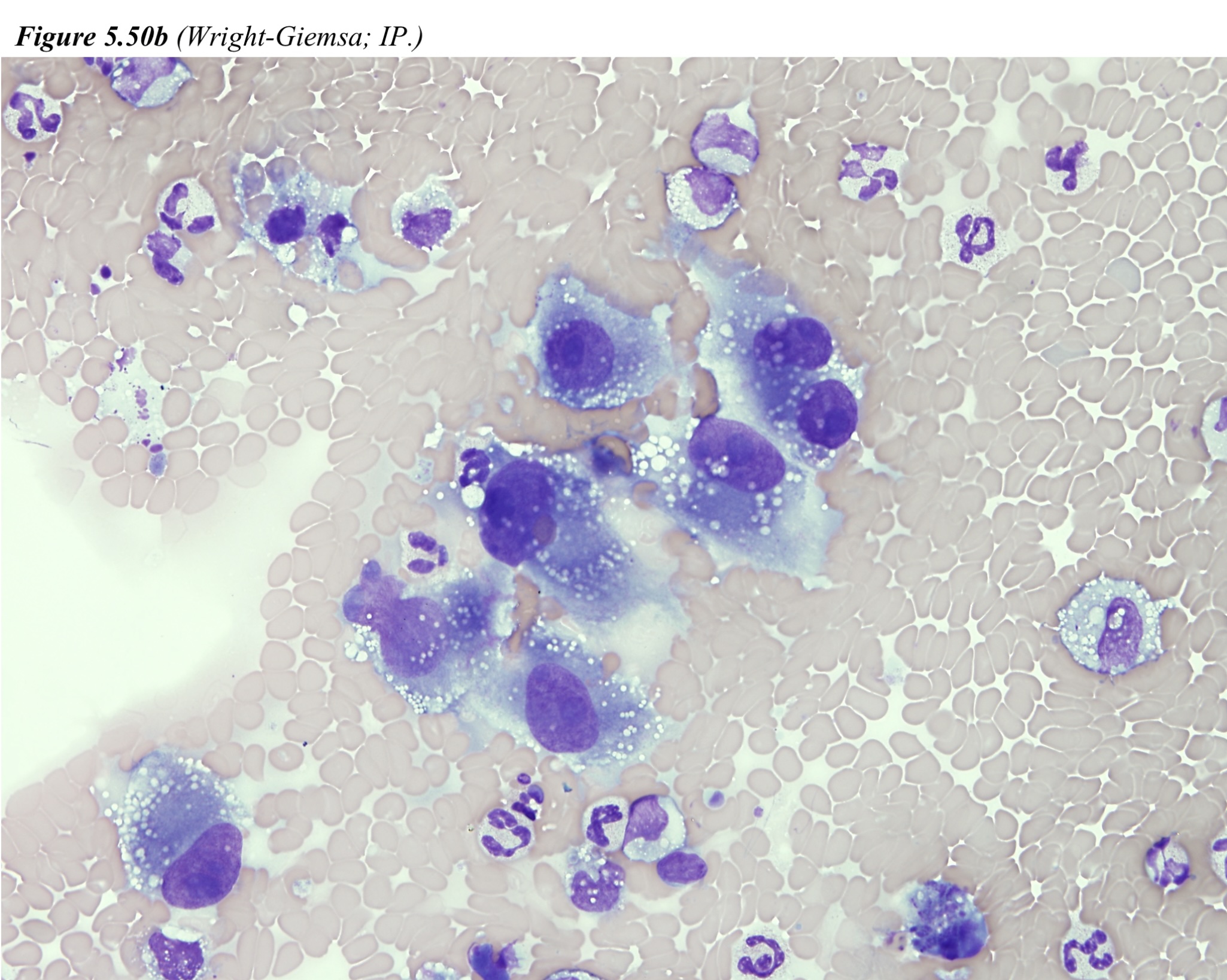
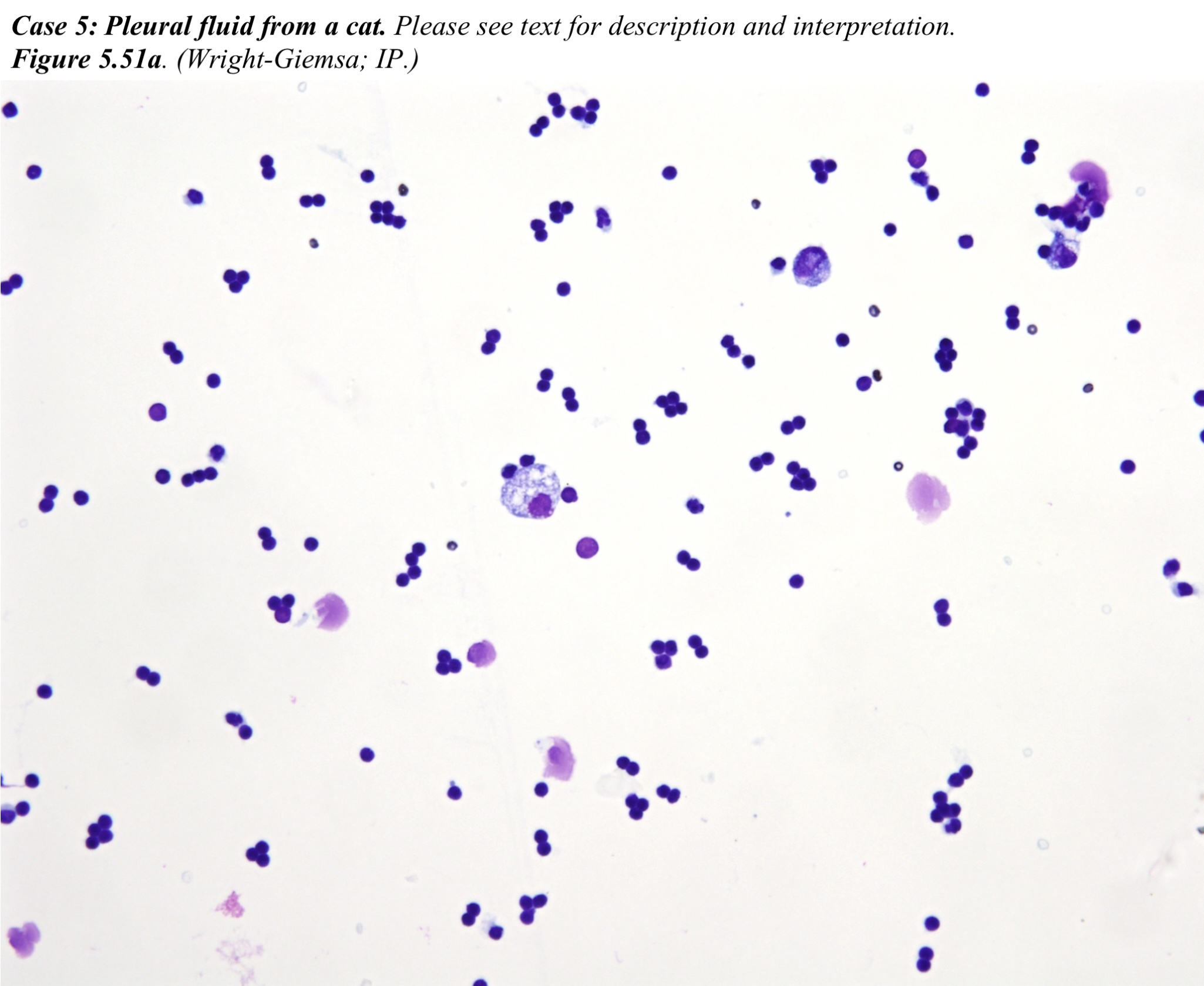
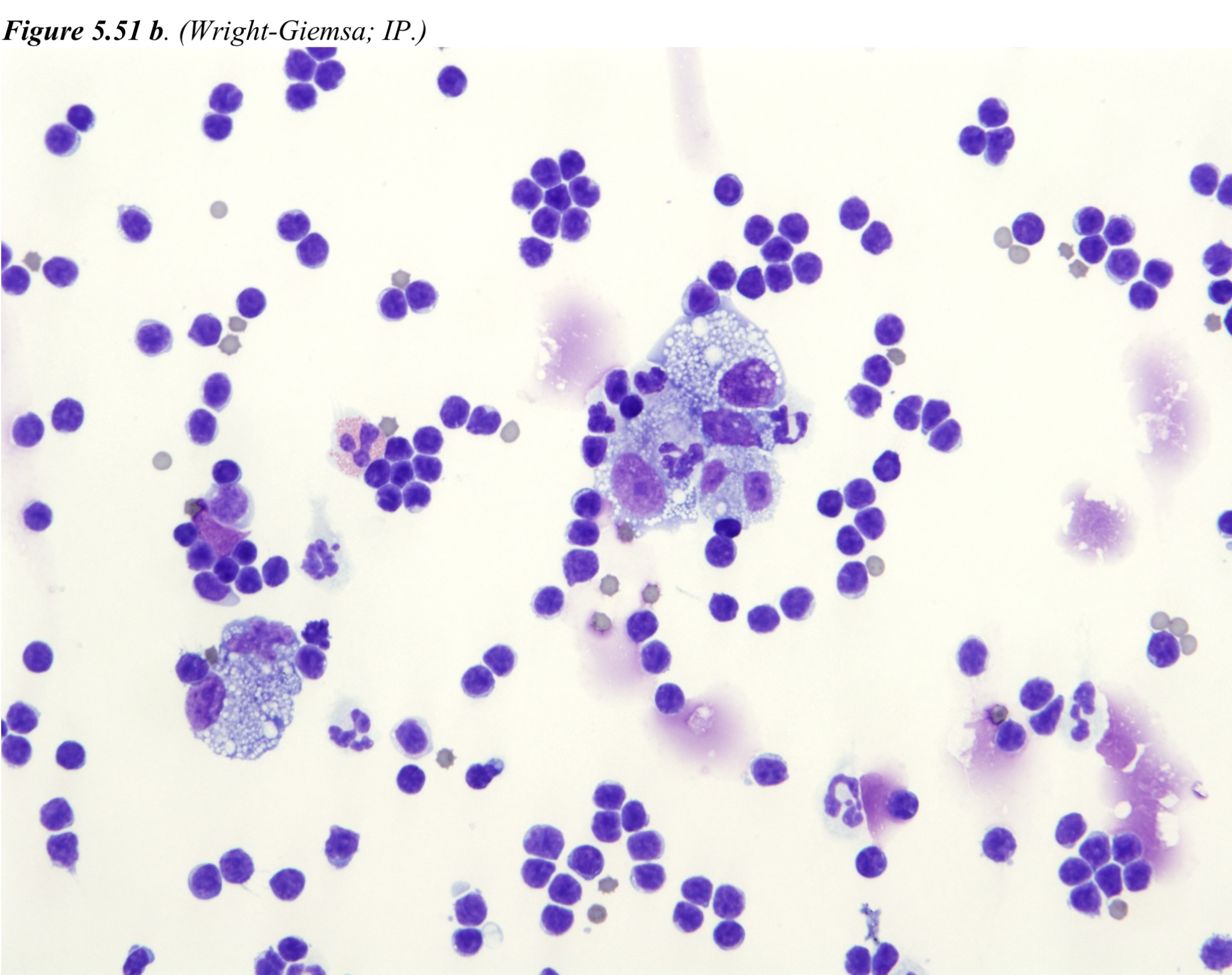
Pleural Fluid
The nucleated cell count is elevated and the protein measurement by refractometry is probably inaccurate due to the milky nature (indicating high lipid content) of the fluid. Most cells are small lymphocytes. Foamy macrophages, nondegenerate neutrophils, mesothelial cells, and rare eosinophils are also seen. Erythrophagia and leukophagia are occasional. These findings are consistent with a chylous effusion (see Fig. 5.35 and Fig 5.36).
TTW
The direct smear is of low cellularity. There are large amorphous clumps of stringy, pale blue material enmeshed with a mixed population of inflammatory cells, epithelial cells, and alveolar macrophages. The cytospin preparation contains several sheets and clumps of uniform, ciliated, columnar epithelial cells. The inflammatory cells comprise eosinophils, macrophages and nondegenerate neutrophils (60:30:10). Macrophages often contain blue globular material, probably mucin.
This is a nonseptic, eosinophil-rich inflammatory process with increased mucus production. These findings support a diagnosis of allergic airway disease (feline asthma).
- Ginny had chronic allergic bronchitis which may have predisposed to the development of chylothorax. There is no further follow-up.
Case 6. Blue
Blue, a 2 year old F Border collie dog, was presented in recumbency with acute neurological signs. The dog has a history of being kicked several times by cattle and horses, and recurrent swelling of the left nasal area with subsequent ocular swelling over the past year. The swelling had been treated 3-4 times with antibiotics and occasionally steroids, and had resolved.
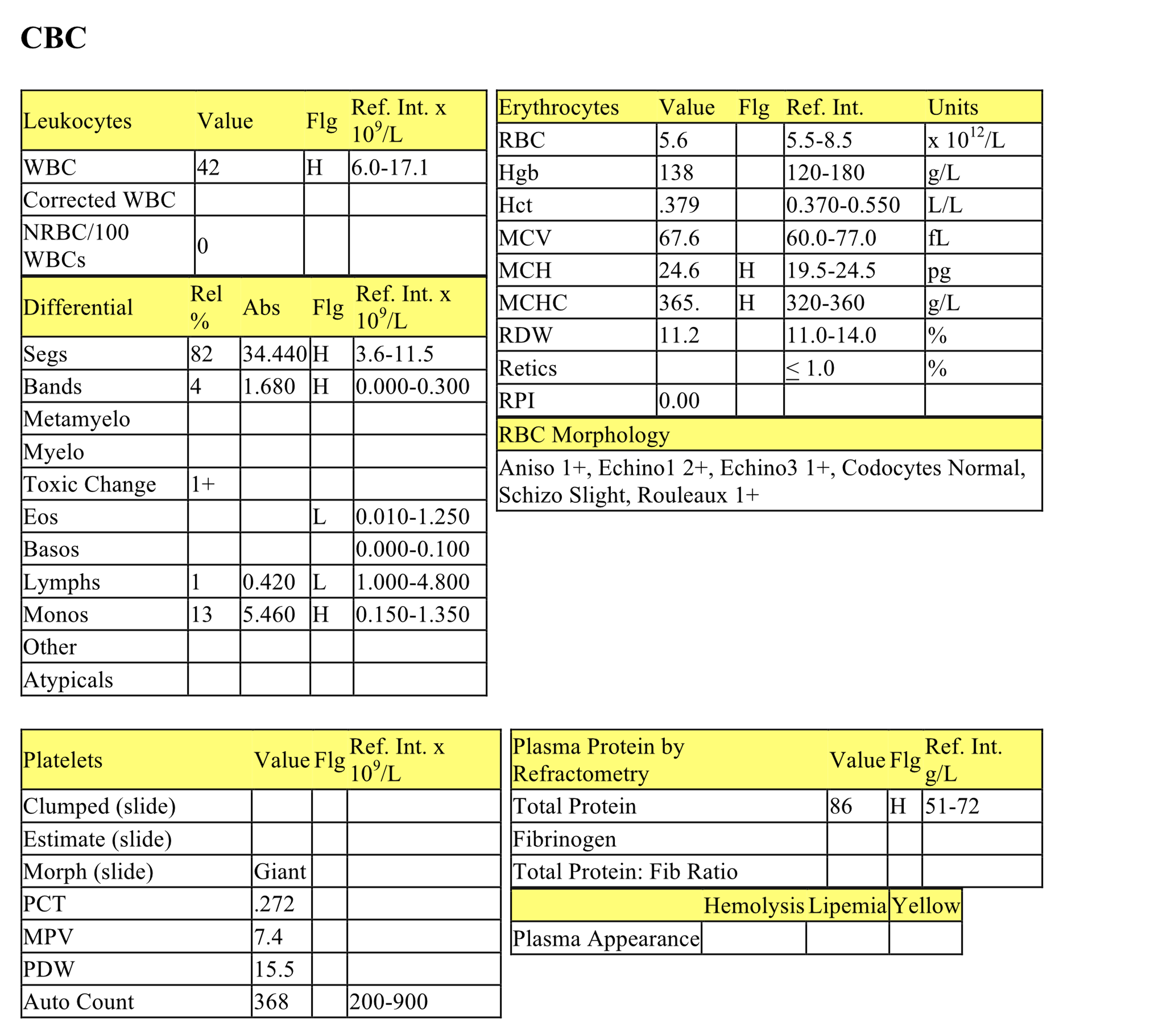
CBC
The hematocrit is low normal which could represent a mild anemia, particularly if Blue was dehydrated upon presentation. Mild anemia could be due to anemia of inflammatory disease. Very mild increases in MCH and MCHC may be due to an increase in hemoglobin (disproportionate compared to RBC count and hematocrit), possibly reflecting some very mild hemolysis (no indication of red plasma). Rouleaux formation may be due to hyperproteinemia. Moderate leukocytosis is characterized by a moderate neutrophilia with a significant left shift, mild toxic change, and moderate monocytosis. The leukogram is consistent with chronic inflammation. Lymphopenia indicates concurrent stress. The protein is inaccurately high on refractometry, probably from the hypercholesterolemia (although there is still a hyperproteinemia on the biochemical panel, but not to the same degree).
Biochemical Panel
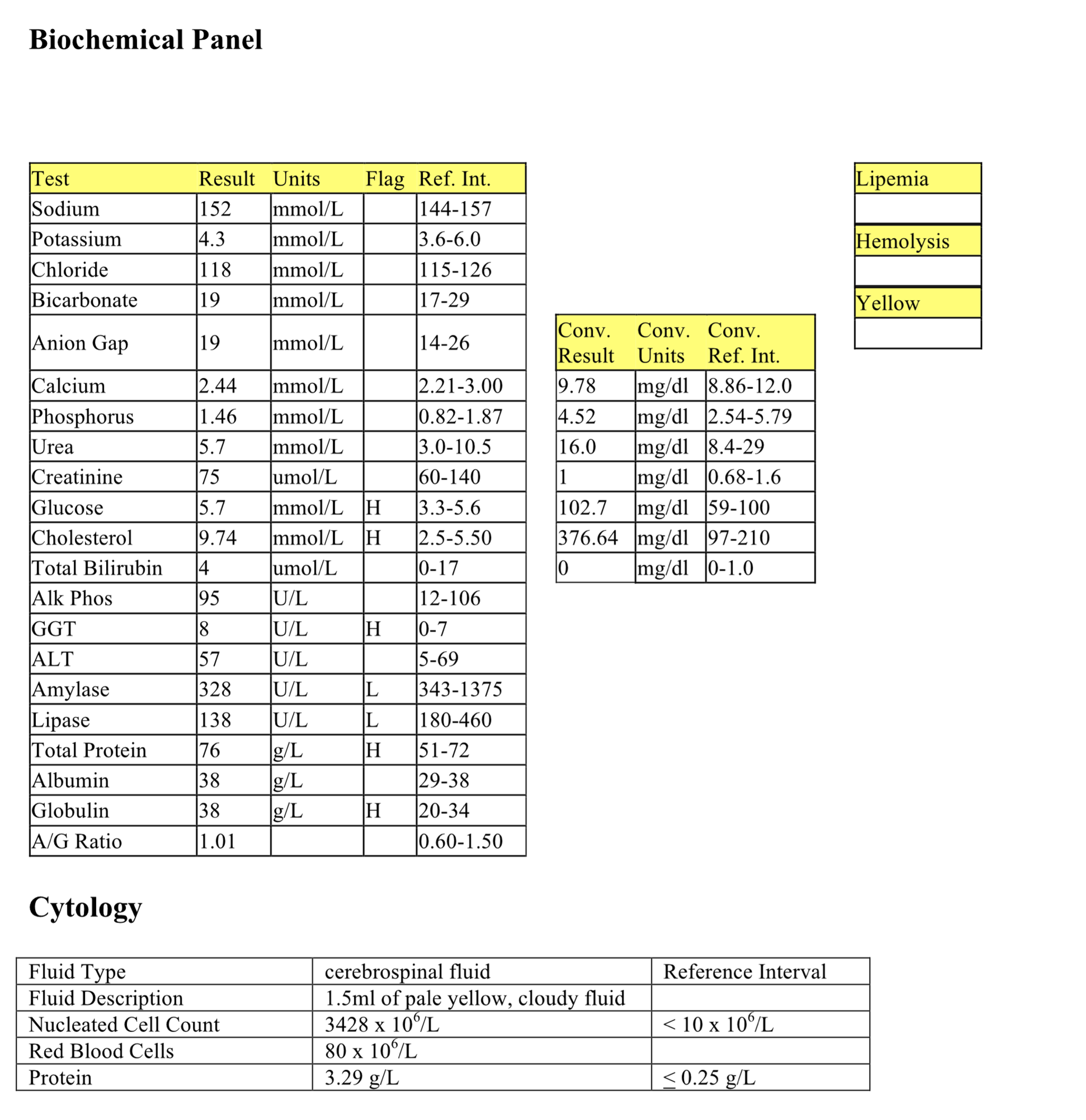
Very mild hyperglycemia may not be significant, but could reflect stress of illness. Mild hypercholesterolemia may be postrprandial or due to cholestasis. Decreased amylase and lipase have no pathologic significance. Mildly increased GGT may not be significant given the normal ALP, but could reflect mild cholestasis. Mild hyperproteinemia, high normal albumin and globulins, and the normal albumin to globulin ratio (indicating panhyperproteinemia) support mild dehydration.
Vitreous Fluid
The vitreous aspirate is highly cellular and degenerate neutrophils predominate. Both short rods and filamentous chains of bacteria are found within neutrophils and extracellularly. These findings indicate marked septic neutrophilic inflammation.
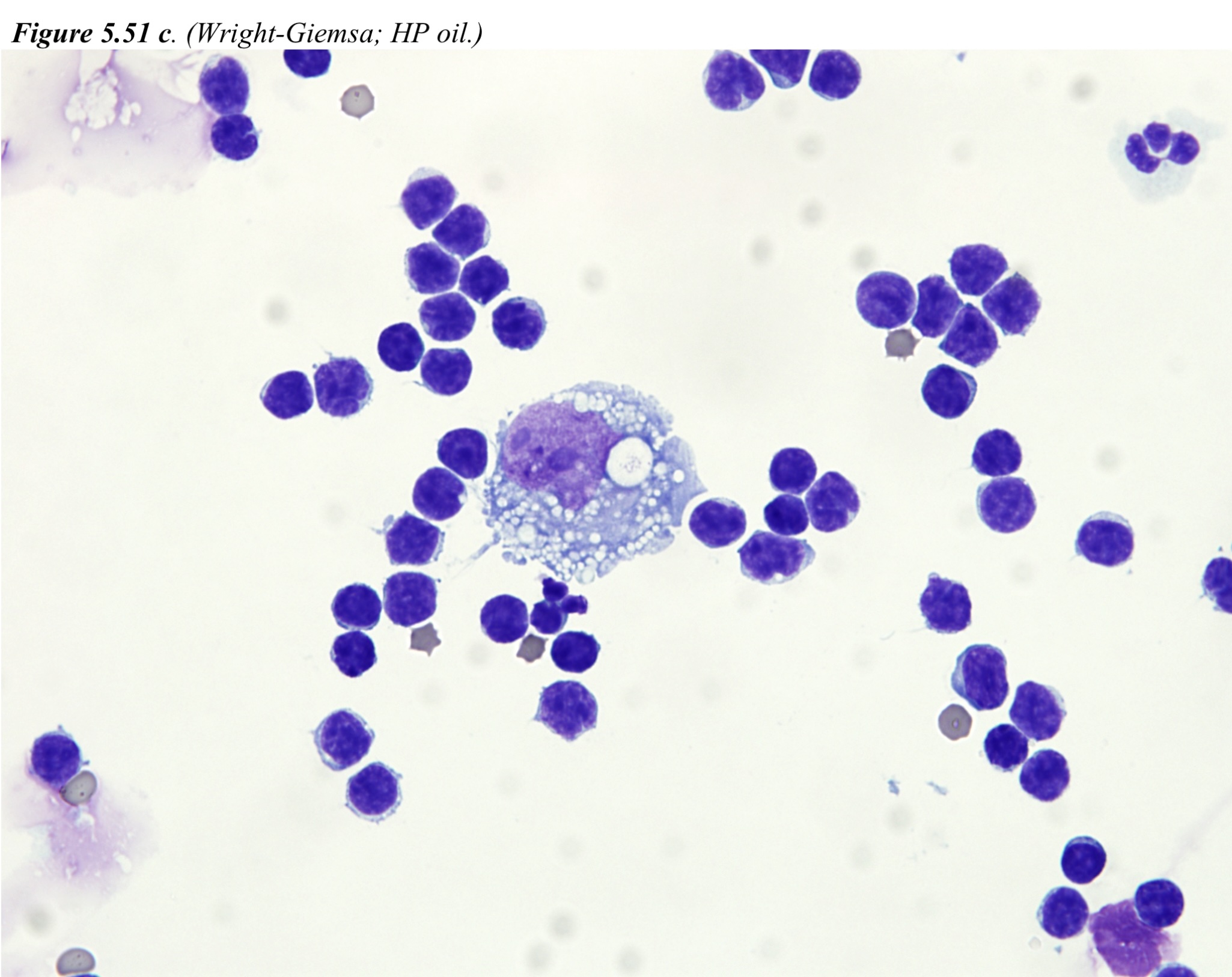
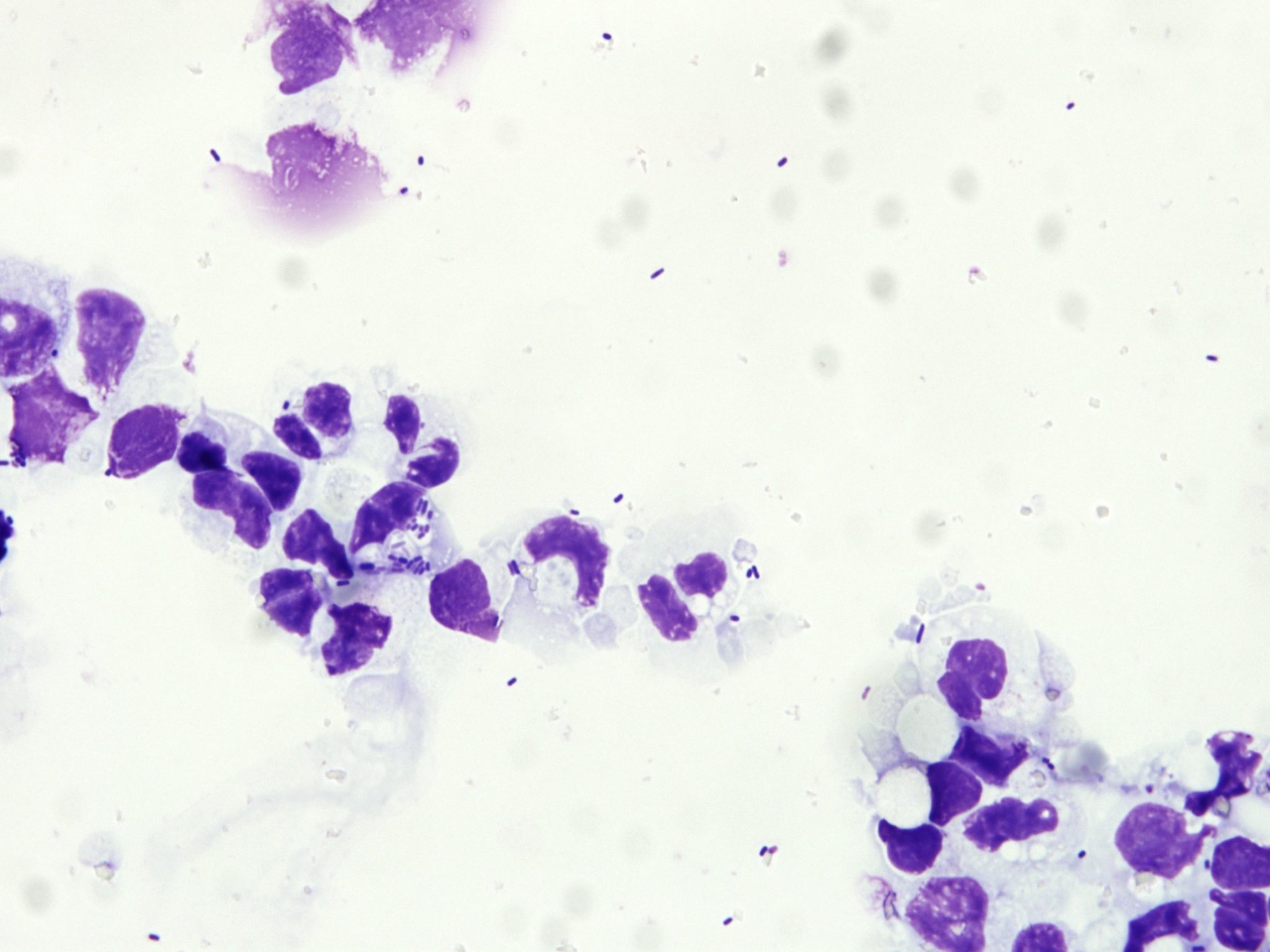
Cerebrospinal Fluid
The nucleated cell count and protein concentration are very high in this CSF. The majority of cells are degenerate neutrophils. Intra- and extracellular bacteria are abundant, both short rods and long, beaded filaments. This fluid represents septic, neutrophilic inflammation and bacterial meningitis. Although the organisms are pleomorphic, they may be all of one type, particularly following antibiotic therapy. Actinomycosis, nocardiosis, and fusobacteriosis would be differentials for the etiologic diagnosis in this case.
- Given the very poor prognosis, Blue was euthanized.
Case 7. Pierre
Pierre, a 6-year-old M Labrador Retriever X dog, was presented with ataxia, lethargy, and anorexia. Abdominal ultrasound revealed an enlarged spleen and abnormal liver.
CBC
There is a mild to moderate anemia that is macrocytic and moderately regenerative. Very mildly decreased MCHC and low numbers of microcytes are likely not significant. Nuclear remnants are secondary to regeneration. The regenerative anemia may be due to blood loss or hemolysis. The leukogram reflects stress and possibly mild inflammation, although the age of the sample makes assessment of bands difficult. Platelets are clumped but estimated to be decreased, although not to the degree noted in the automated platelet count. See biochemical panel for interpretation of hypoproteinemia.
Biochemical Panel
Moderate increases in bilirubin and slightly yellow serum may be due to increased extravascular hemolysis, but given the increased ALP activity, cholestasis cannot be ruled out. Increases in ALT and GLDH activity reflect hepatocellular injury. There is essentially a panhypoproteinemia (globulins are low normal, normal A/G ratio) that may be due to protein loss into the GI tract, but blood loss could also contribute to a panhypoproteinemia. Part of the hypoalbuminemia may reflect albumin’s role as a negative acute phase protein.
Urinalysis
3+ bilirubin and scant bilirubin crystals reflect hyperbilirubinemia.
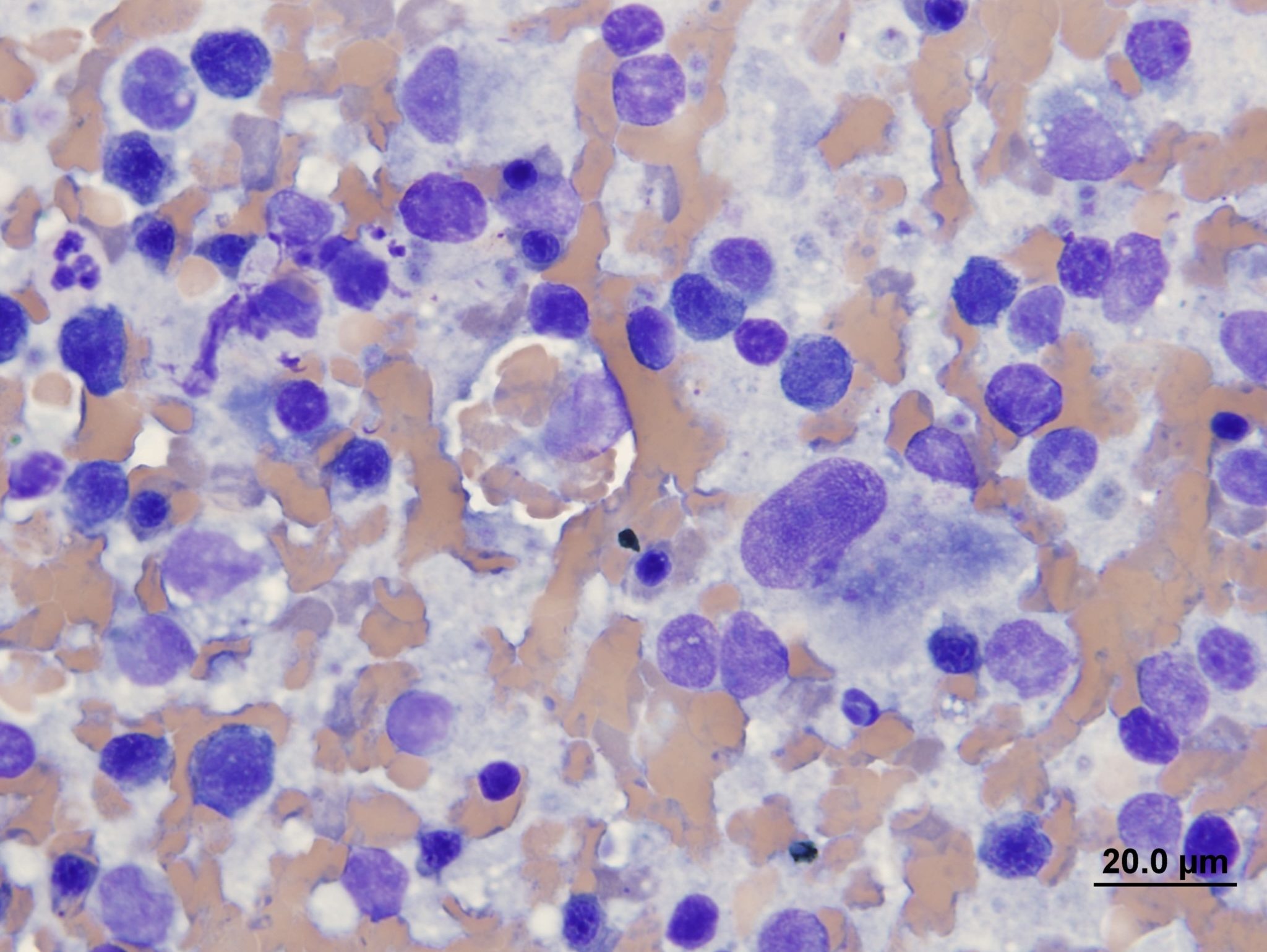
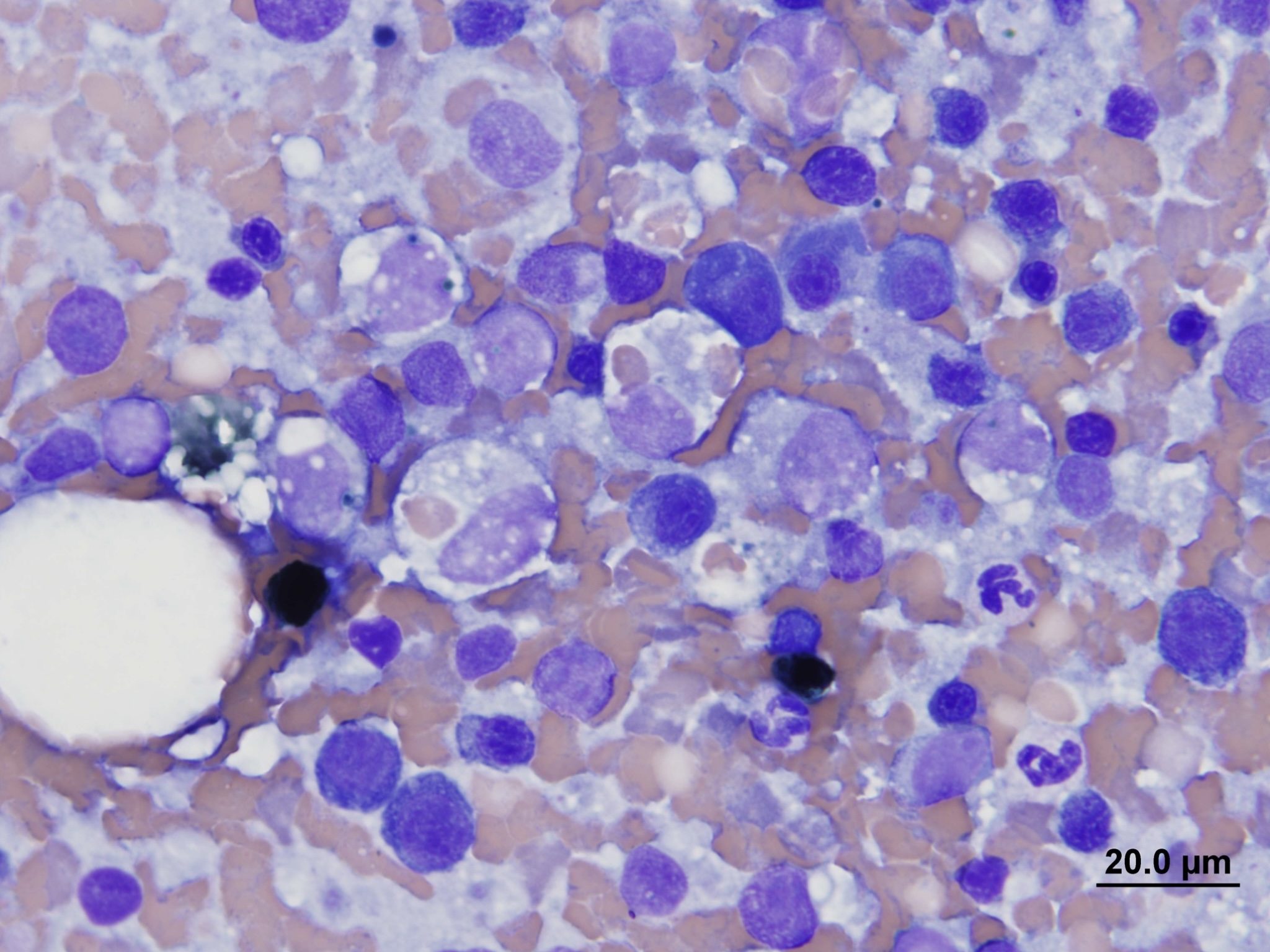
Splenic Aspirates
Aspirates from the spleen are highly cellular and contain numerous large erythrophagocytic histiocytes that have also occasionally phagocytosed platelets. Histiocytes display moderate anisocytosis and anisokaryosis and have prominent nucleoli. Occasional cells contain dark green granules consistent with hemosiderin. There is abundant peripheral blood in the background, as well as lymphocytes and low numbers of hemopoietic precursors (reflecting extramedullary hematopoiesis). Pierre was diagnosed with histiocytic sarcoma.
- Histiocytic sarcoma with phagocytosis of erythrocytes and platelets is responsible for the anemia and the thrombocytopenia. The liver was also infiltrated by neoplastic histiocytes, resulting in the changes on the biochemical panel.
- Pierre was sent home and treated with chemotherapy. No further follow-up is available.
Case 8. Daisy
Daisy, a 3-year-old F(s) domestic shorthair cat, has a lytic lesion on the right distal radius and a 3-4 week history of right forelimb lameness.
Bone Aspirate
Aspirates are highly cellular and contain a population of individual round to spindle cells with round nuclei on a background of abundant peripheral blood. Cells have moderate to abundant basophilic granular cytoplasm that may contain eosinophilic material. Cells display moderate to occasionally marked anisocytosis and anisokaryosis. Cells have multiple prominent nucleoli and are occasionally binucleate. Cytologic findings are highly suggestive of osteosarcoma.
- Osteosarcoma was confirmed by histology.
- The right forelimb was amputated and Daisy was sent home.
Case 9. Skit
Skit, a 2-year-old M(c) mixed breed dog, was presented for a red, raised mass on the R pinna.
Mass Aspirate
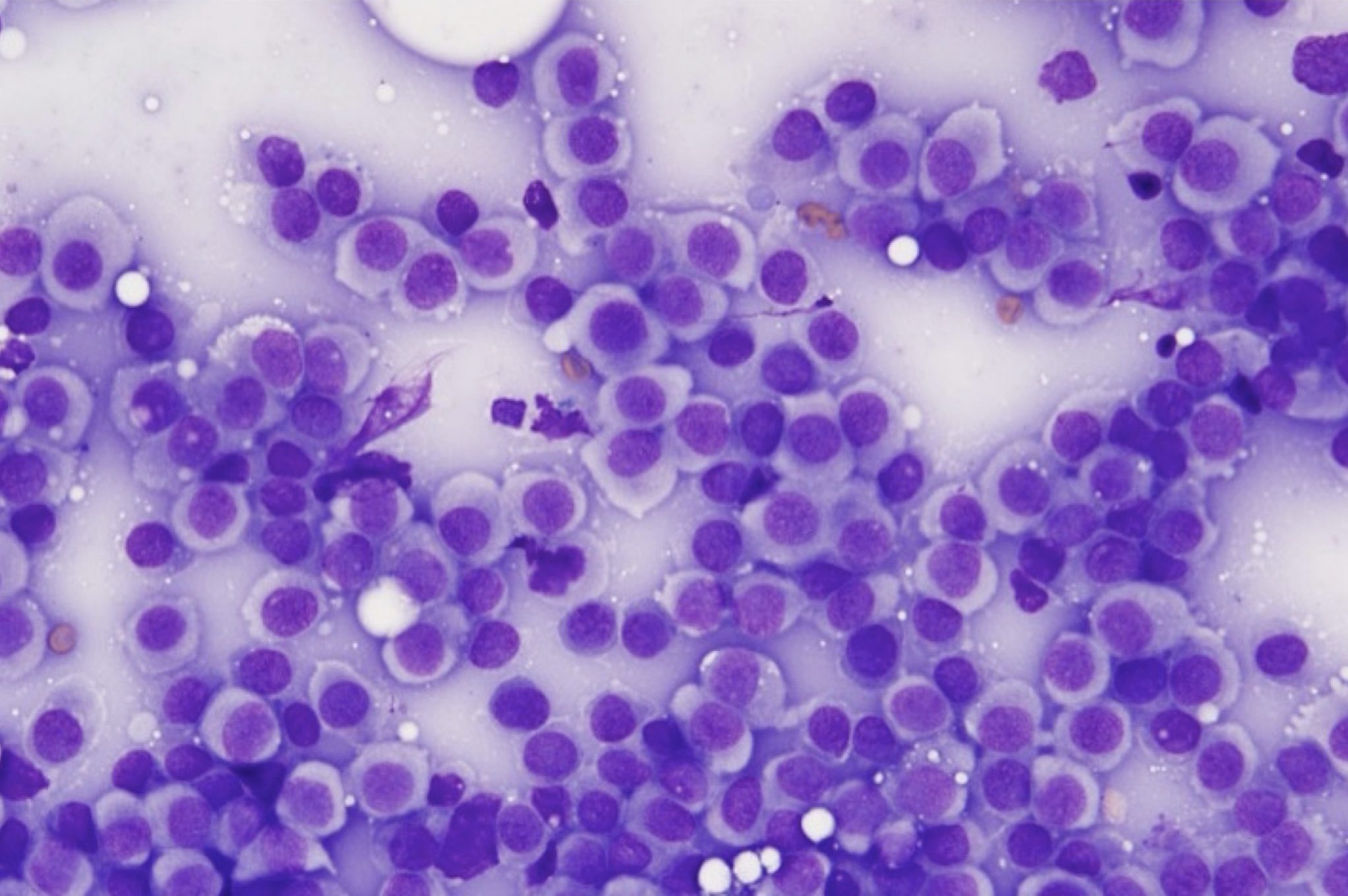
Aspirates from the mass are highly cellular and contain a uniform population of discrete round cells. Cells have round nuclei with a finely stippled chromatin pattern, and a moderate amount of pale cytoplasm, typical of histiocytes. Cells display mild anisocytosis and anisokaryosis.
- Skit was diagnosed with a cutaneous histiocytoma. The histiocytoma regressed spontaneously without intervention.
Case 10. Tex
Tex, a 7-year-old M(c) Labrador Retriever dog, has a history of hematuria and pollakiuria. Abdominal ultrasound revealed thickening at the trigone of the bladder.
Bladder Mass Traumatic Catheterization
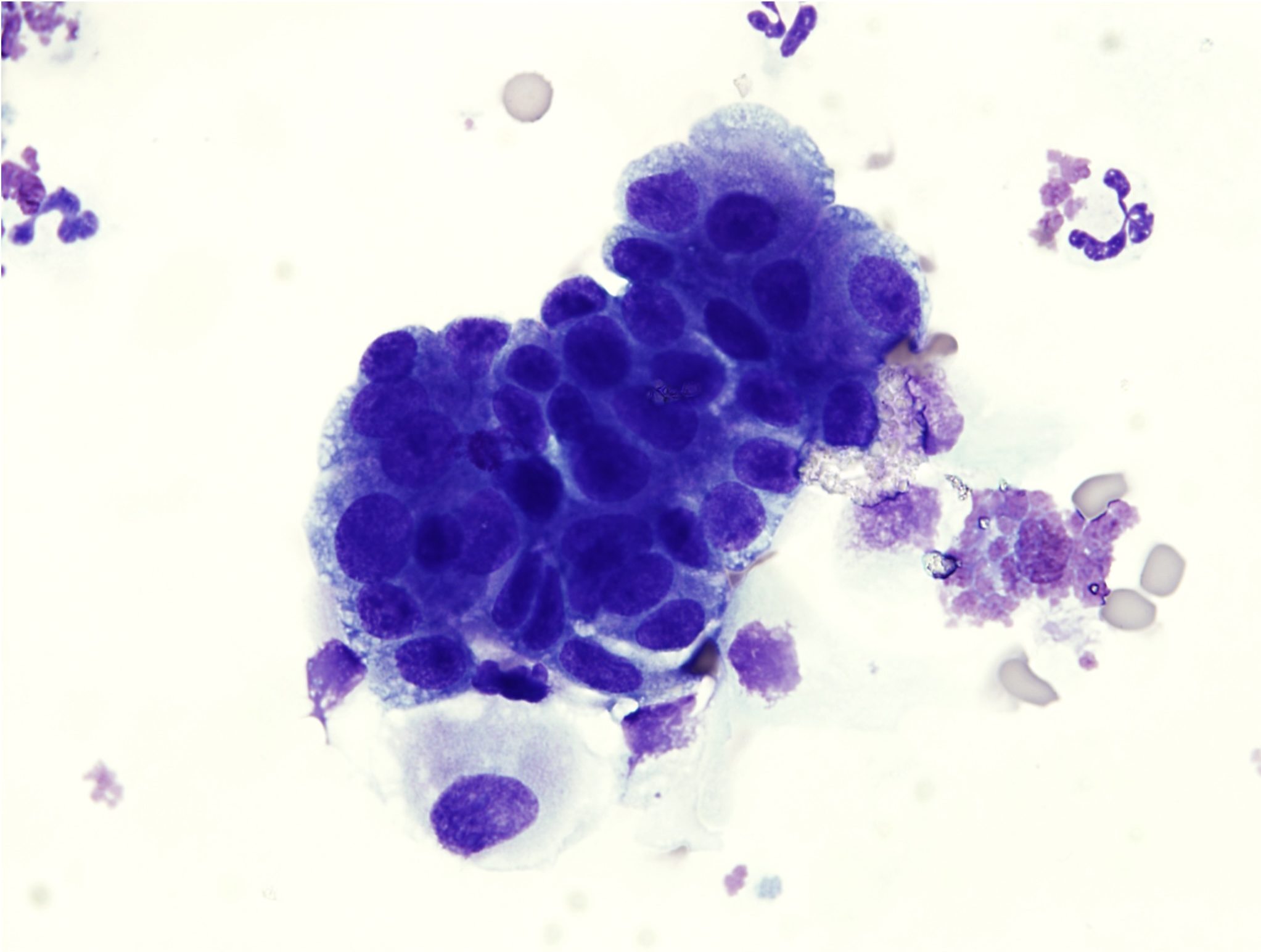
Aspirates are highly cellular and contain numerous clusters of atypical epithelial cells. Cells display marked anisocytosis and anisokaryosis and have a variable N:C ratio. The cytoplasms range from deeply basophilic to pale and vacuolated. Cells have multiple prominent nucleoli and occasionally display nuclear molding. These cells are typical of transitional cell carcinoma.
- The prostate was also enlarged and mineralized. Similar neoplastic cells were found in samples from the prostate.
- No further follow up is available.
Additional Cases
Chapter 3: Hemopoietic Neoplasia
Jaundice; deposition of pigment in skin, mucous membranes and sclera due to hyperbilirubinemia; usually results in a yellow discoloration of skin and mucous membranes.
All tests on the complete blood count (CBC) that evaluate erythrocytes, including morphologic examination on the peripheral blood smear.
Oxygen-carrying molecule within erythrocytes.
Erythrocyte with even projections all around its membrane; often an artifact but can be a pathologic change. Echinocytes are classified as types 1 and 3 depending on the length and sharpness of the projections (spicules).
Increase in the number of neutrophils in peripheral blood.
Release of less mature neutrophil stages (bands, metamyelocytes, myelocytes) from the marrow into the peripheral blood in response to inflammation.
Increases serum urea and/or creatinine.
Impaired bile flow.
Most abundant plasma protein in health; maintains oncotic pressure.
Concurrent decreased concentration of albumin and globulins.
Technique for separating and quantitating proteins in fluids, e.g. serum or urine.
Gammopathy characterized by a broad-based peak in the gamma region and reflecting production of many different immunoglobulins from antigenic stimulation as may be seen with a chronic infection.
Volume of erythrocytes per liter of whole blood. Reported as L/L (calculated: MCV x RBC count). Equivalent to PCV (%) determined by centrifugation of blood in a microhematocrit tube
Average erythrocyte size in femtoliters (measured or calculated PCV or Hct÷RBC).
Average amount of hemoglobin per erythrocyte (calculated: hemoglobin÷RBC count).
Average concentration of hemoglobin per erythrocyte (calculated: hemoglobin÷hematocrit).
Increased number of erythrocytes with decreased volume that usually corresponds with decreased MCV; often associated with iron deficiency as well as portosystemic shunts.
Nonspecific term for sublethal or lethal injury to hepatocytes due to various causes, e.g. hypoxia, toxins, infection.
Azotemia due to renal disease.
Erythrocyte rupture or destruction; may occur in vitro or in vivo as a pathologic process.
Constellation of: retention of metabolic waste products, acid-base and electrolyte disturbances, and compromised urine concentrating ability that develops when the functional mass of the kidneys is reduced by 70% or more; may be acute or chronic.
Method of urine collection involving insertion of a needle directly into the urinary bladder via the abdominal cavity, bypassing the lower urinary tract.
Decrease in hematocrit (PCV) recognized on the complete blood count (CBC); usually hemoglobin concentration and RBC numbers are also decreased.
See Secondary hemostasis.
Process in which fibrin is broken down, resulting in clot dissolution.
Disseminated Intravascular Coagulation & Fibrinolysis; simultaneous disorders of coagulation and fibrinolysis due to generalized derangement of hemostasis.
Erythrocyte with little central pallor and several irregular membrane projections.
Crescent-shaped cells that are formed from mechanical shearing (usually due to fibrin strand deposition) of the red cell.
An erythrocyte fragment created by shearing trauma to erythrocytes within the vascular system; often the fragment which has been sheared off to form a keratocyte.
Decrease in the number of circulating platelets below the reference interval.
Difference between unmeasured anion and cation concentrations, calculated using the formula: (Na+ + K+) minus (Cl- + HCO3-.)
Azotemia due to extracellular fluid volume depletion (dehydration).
Partial thromboplastin time; diagnostic test used to evaluate the intrinsic and common pathways.
Fibrin/fibrinogen Degradation Products; increased concentration of these products supports a diagnosis of DIC&F.
Prothrombin time; diagnostic test used to evaluate the extrinsic and common pathways.
Pinpoint hemorrhage visible on superficial surfaces such as oral mucosa and less-haired skin of animals with thrombocytopenia or platelet function defects.
Number of erythrocytes per liter of whole blood (measured).
“Stack” of red blood cells resembling a roll of coins; prominent in equine and often feline blood. Formation increases as negative charges between RBCs decrease (e.g. with increased plasma proteins).
Increase in the number of monocytes in peripheral blood.
Piece of the nucleus that persists in the mature erythrocyte. May be seen in healthy animals, especially cats, and those with regenerative anemias, or hypofunctioning spleens.
Erythrocyte destruction within macrophages of the spleen, liver, lymph nodes, and bone marrow; often accompanied by hyperbilirubinemia and bilirubinuria.
General term for a decrease in number of any cell line in peripheral blood.
