
Appendix I: Practice Cases
Case 1. Katarina
Katrina, a 4-year-old F(s) Siberian Husky dog, had a productive cough and mucopurulent nasal discharge for several weeks. A transtracheal wash revealed pyogranulomatous inflammation and blastomycosis.
Case 2. Thor
Thor, a 6-year-old male Lhasa Apso x dog, was inappetent and lethargic for 6 days, and then started convulsing on the morning of presentation to the clinic. On physical examination, he was hypothermic.
Case 3. Wally
Wally, a 12-year-old M(c) DSH cat, became acutely recumbent, and had cold, weak hind legs on physical examination.
Case 4. Ronaldo
Ronaldo, a 9-year-old F(s) Beagle x dog, was presented with polydipsia and polyuria.
Case 5. Dan
Dan, a 9-year-old Quarter Horse gelding, was presented with watery diarrhea of 3 days’ duration. He was depressed, tachycardic, and dehydrated.
Case 6. Zack
Zack, a 7-year-old Male Weimaraner dog was brought in to the emergency service recumbent with blood in the rectum. Tested negative for Parvovirus.
Case 7. Sauron
Sauron, a 2 ½-year-old M(c) English Spaniel dog, had previous episodes of hemolysis and pigmenturia. Previous CBC had reticulocytosis and microcytosis, but no anemia. He had been receiving prednisone therapy for presumed immune-mediated hemolytic anemia. Doing well now.

Interpretations for Practice Cases
-
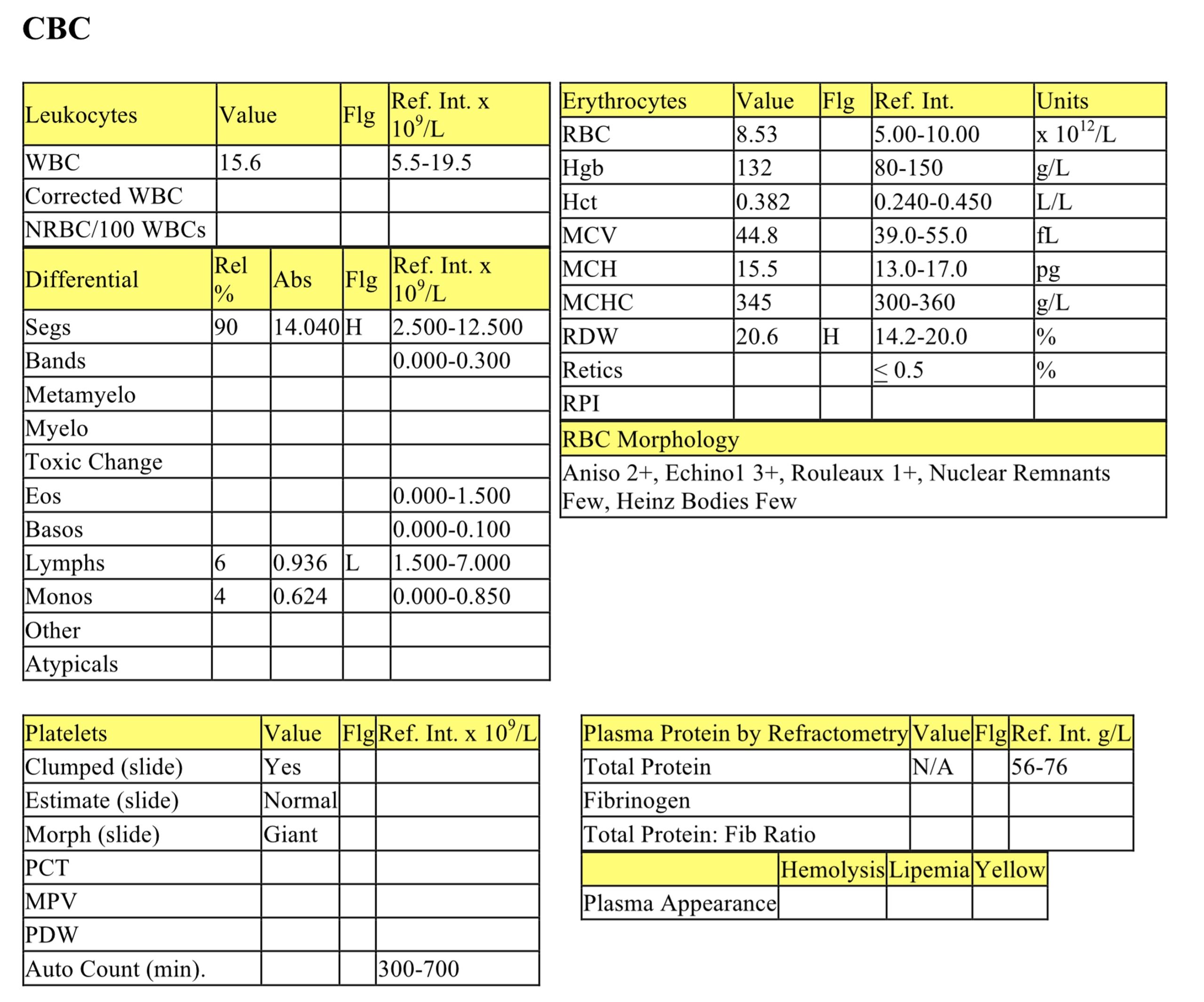
Katarina
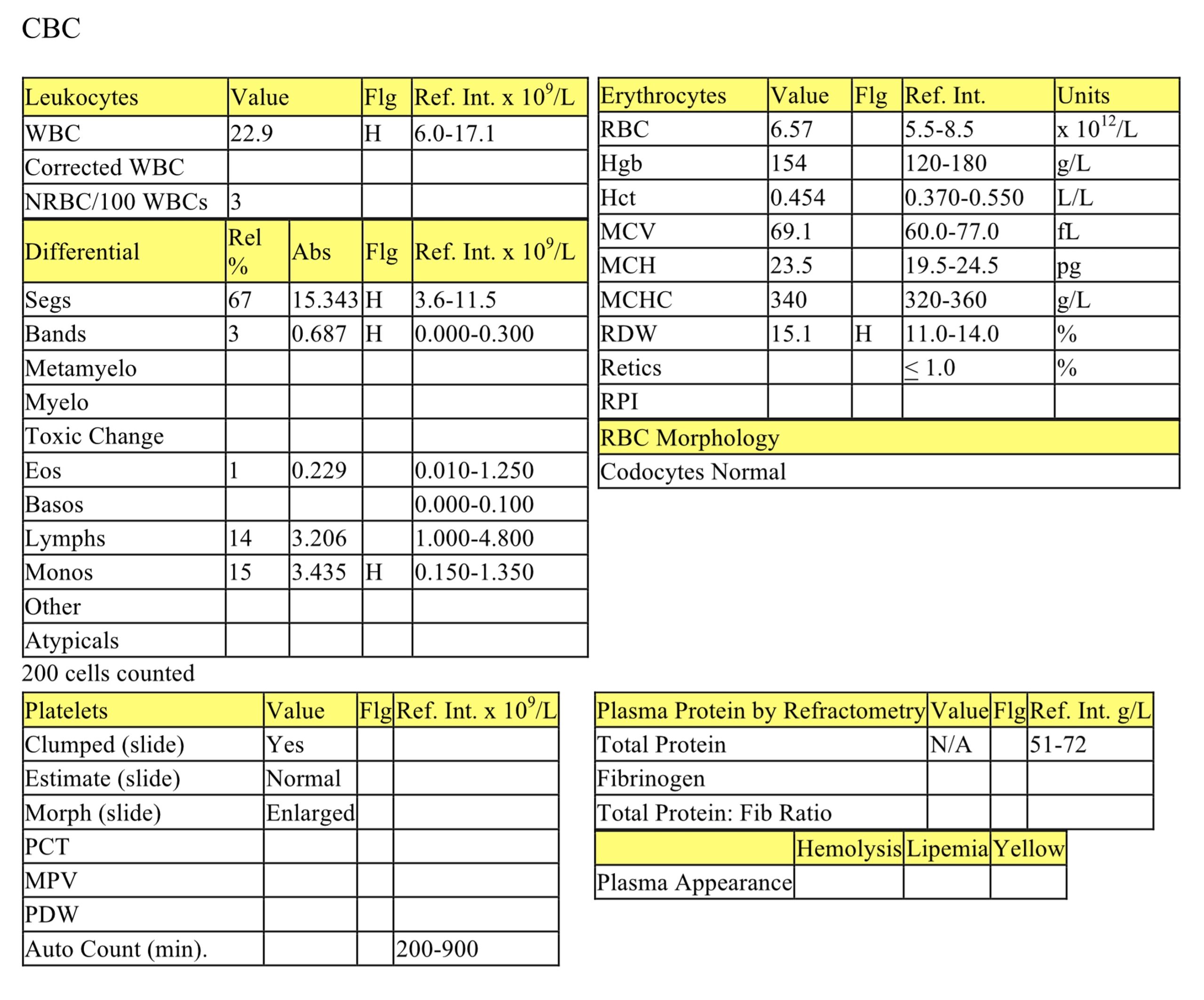
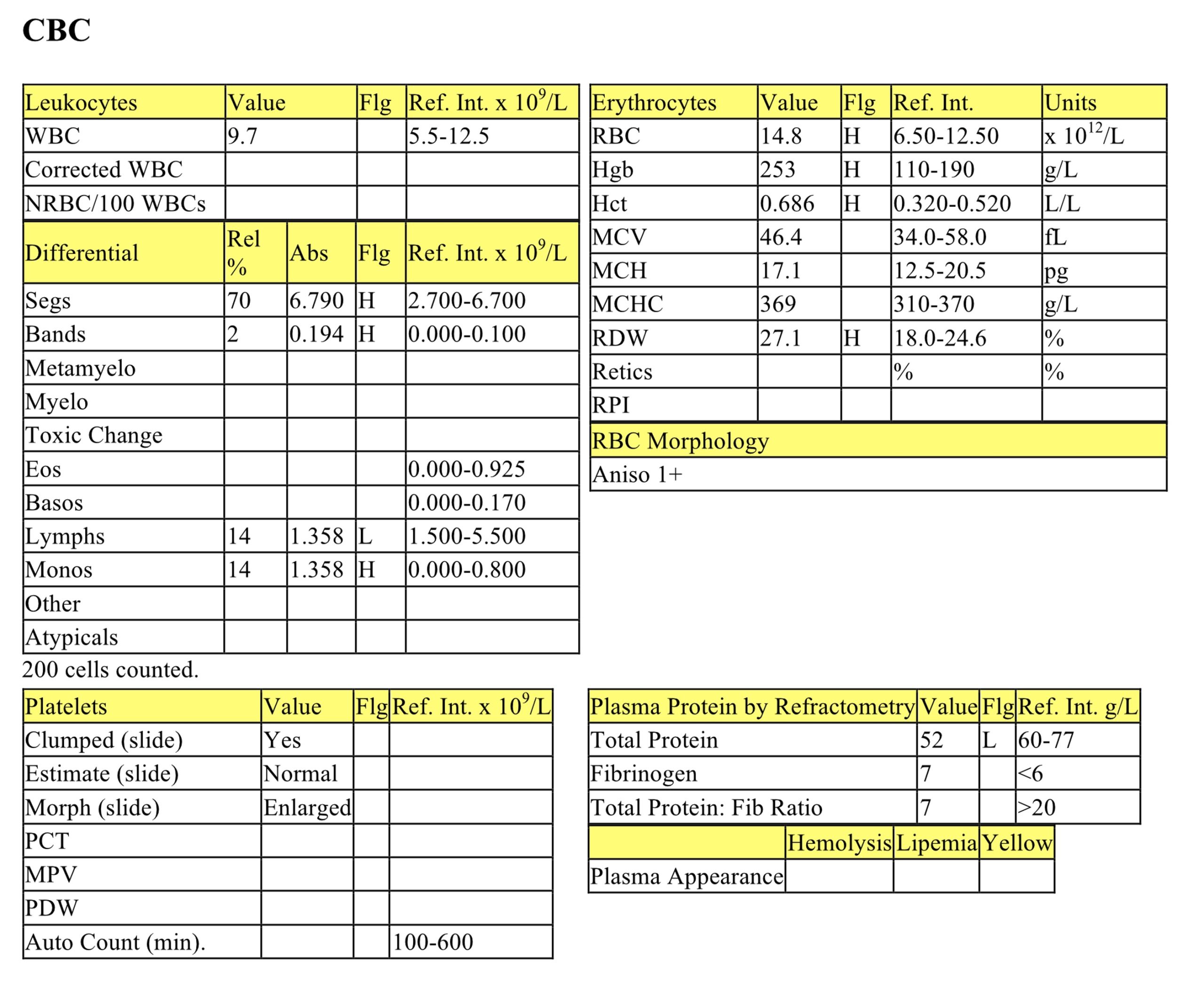
CBC
The erythrogram is unremarkable. The mild increase in RDW does not correlate with increased anisocytosis and is unlikely to be significant. The mild leukocytosis is characterized by a mild neutrophilia, mild left shift, and mild to moderate monocytosis. These leukogram findings suggest an established inflammatory response, likely associated with blastomycosis infection. Lymphocyte numbers are within the RI; there may be no stress lymphopenia because of the chronicity of the infection, i.e., Katarina may not be particularly stressed at this time. Also, there could be chronic antigenic stimulation occurring due to the long-standing infection; this could counteract the effect of cortisol on lymphocyte numbers.
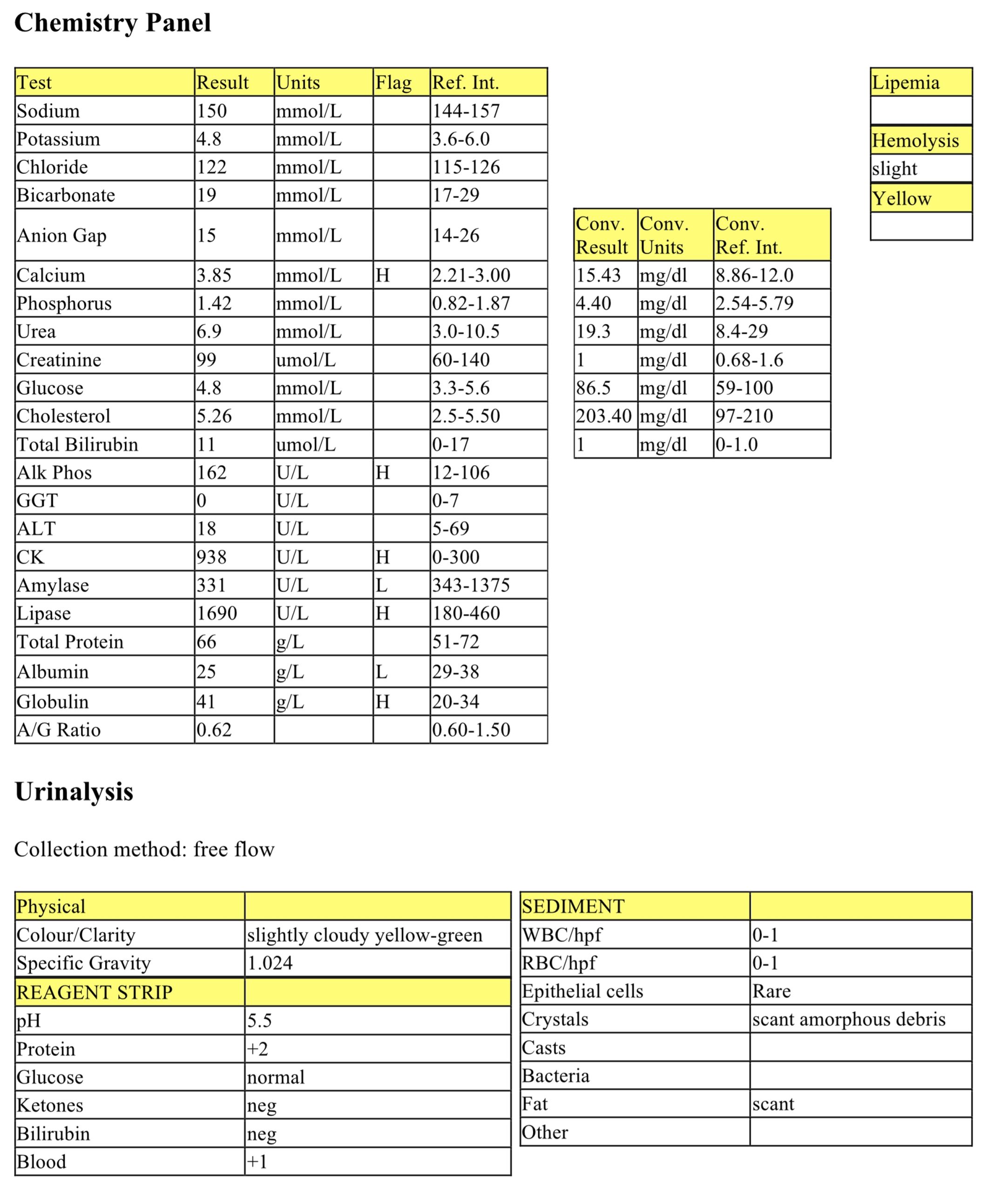
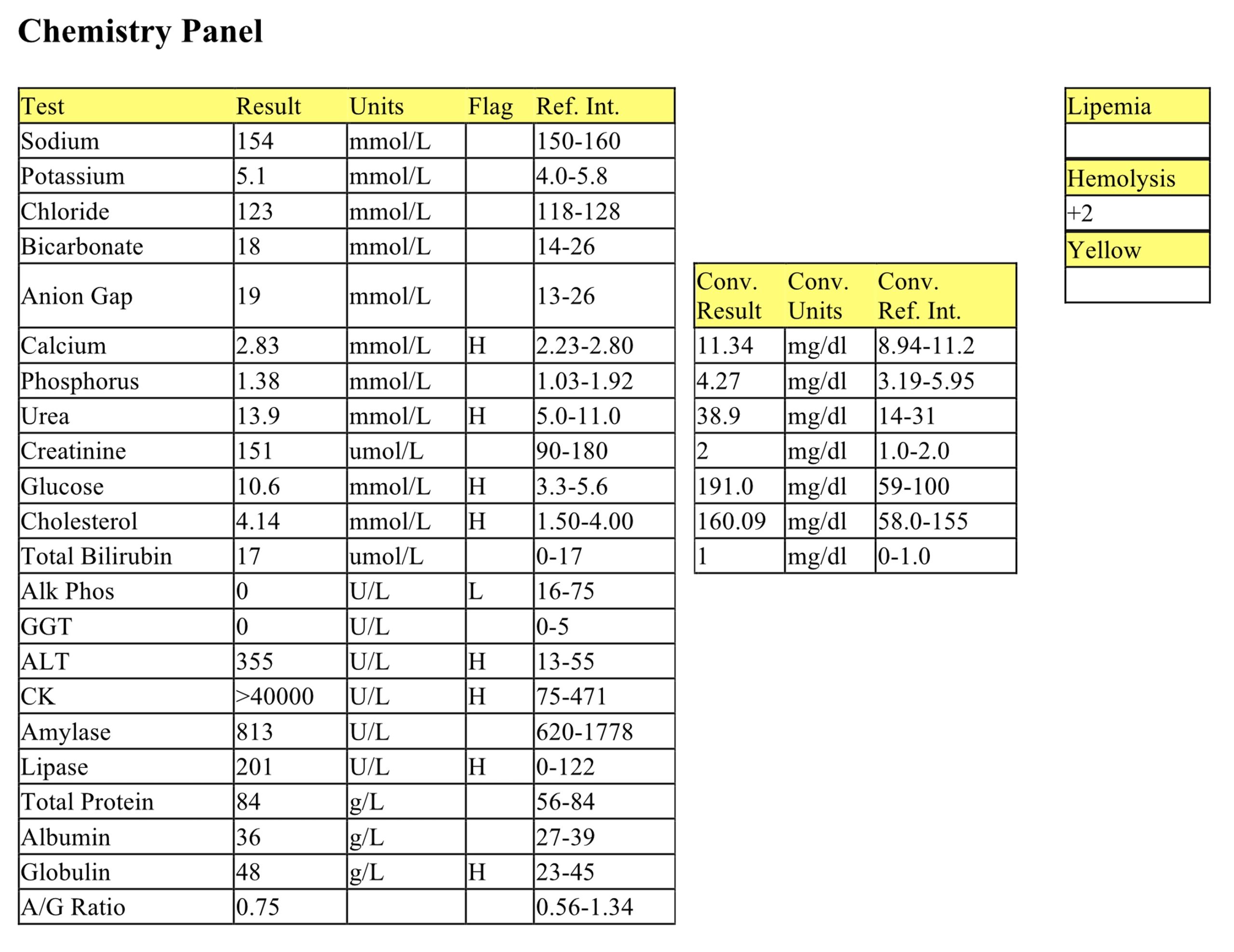
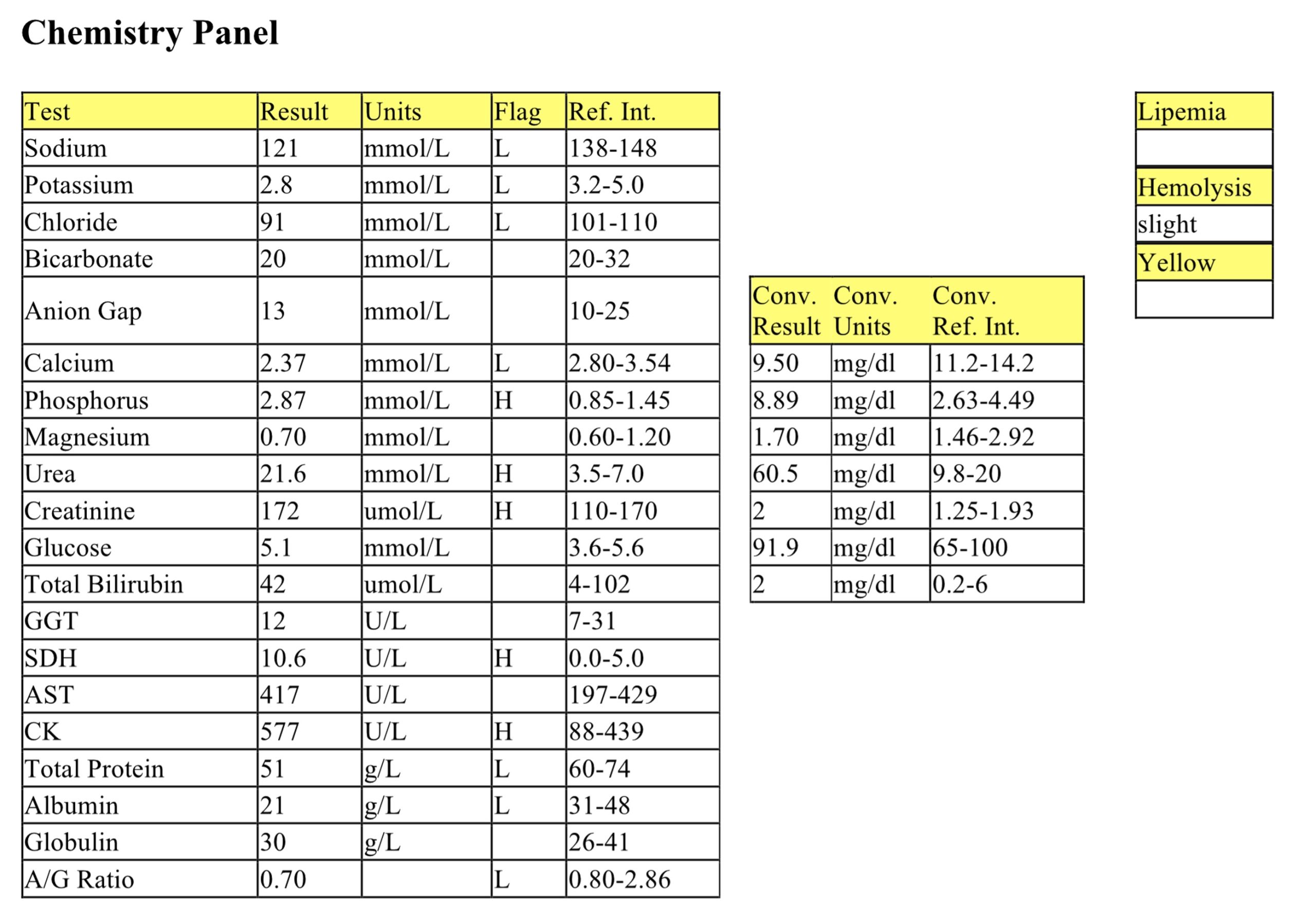
Biochemical Panel
The moderate hypercalcemia can be attributed to Katarina’s history of pyogranulomatous inflammation due to blastomycosis. Blastomycosis stimulates macrophages to produce excess amounts of vitamin D. Vitamin D then stimulates calcium release by bone resorption. Note that while blastomycosis is associated with hypercalcemia, it is not a reliable indicator as many infected dogs may not show this elevation. The mild increase in ALP activity may be attributed to various sources such as cholestasis, enzyme induction (particularly if the animal is chronically stressed and releasing increased levels of cortisol), or more rarely from a bone source. Higher elevations of ALP activity could be seen if the fungal infection involves bone, causing lysis. The mild elevation of CK activity is likely associated with myocyte leakage from venipuncture and handling. Amylase activity is mildly decreased but the general rule is a decrease in enzyme activity is not clinically significant. Lipase activity is mildly to moderately increased, but this is likely not clinically significant in this case, particularly given the lack of clinical signs referable to the pancreas and digestive tract. The lipase activity could be of non-pancreatic source. The mild hypoalbuminemia paired with the mild hyperglobulinemia could be explained by inflammation: hypoalbuminemia through its role as a negative acute phase protein and hyperglobulinemia associated with the activation of positive acute phase proteins and immunoglobulin production due to chronic antigen stimulation and increased acute phase proteins.
Urinalysis
The UA is mostly unremarkable with one exception: +2 protein was noted despite the urine not being concentrated. Paired with the quiet urine sediment (no presence of cells, bacteria or other protein sources), Katarina is a good candidate to recommend a urine protein to creatinine ratio test to determine if there is a significant proteinuria. Chronic infection with blastomycosis could result in antigen-antibody deposition in glomeruli leading to glomerulonephritis and secondary proteinuria.
-
Thor
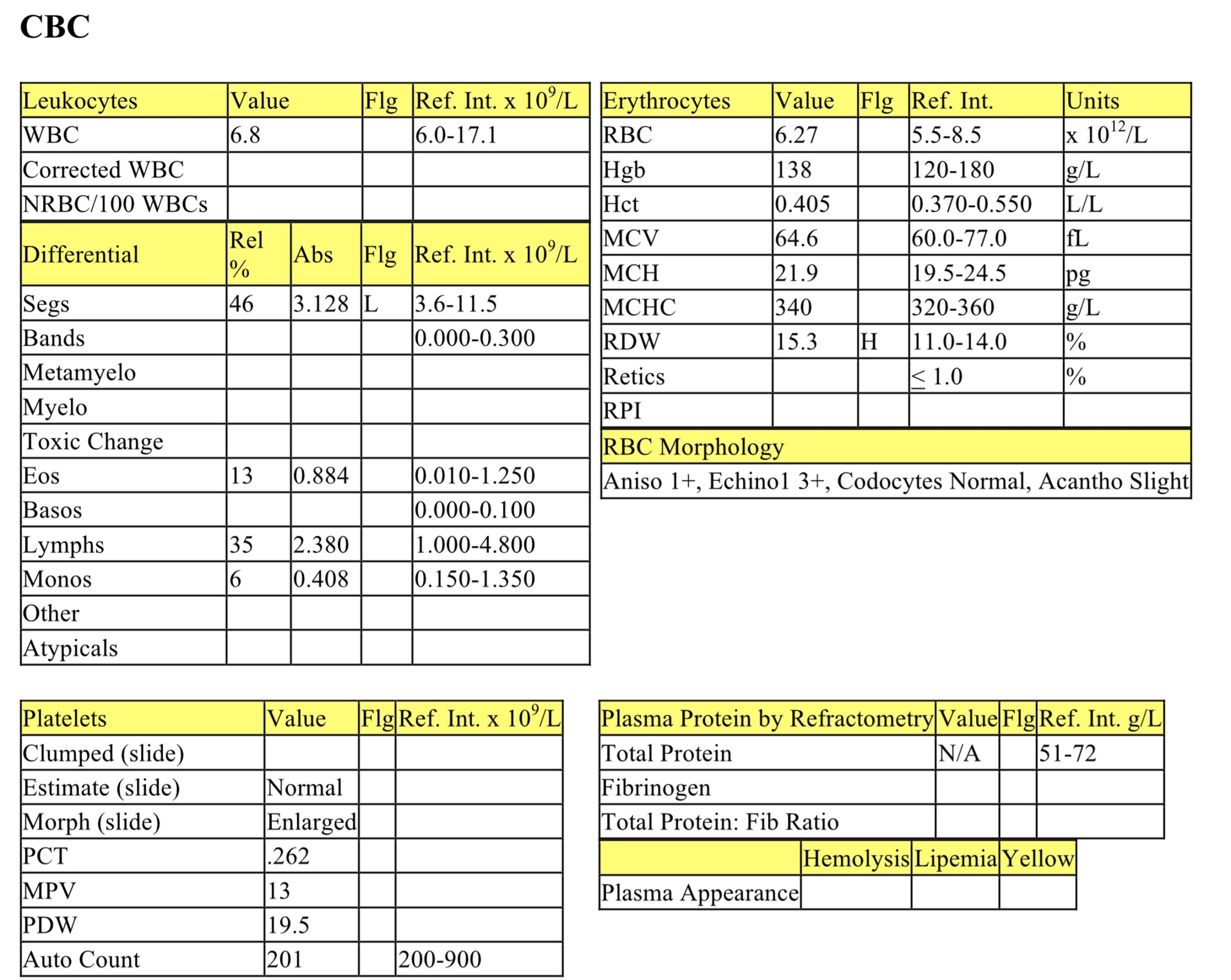
CBC
The erythrogram is unremarkable. The mild increase in RDW does not correlate with increased anisocytosis and is unlikely to be significant. Despite being very ill for six days Thor has a mild neutropenia, high normal eosinophils, and lacks a typical stress lymphopenia. These responses could support a diagnosis of hypoadrenocorticism.
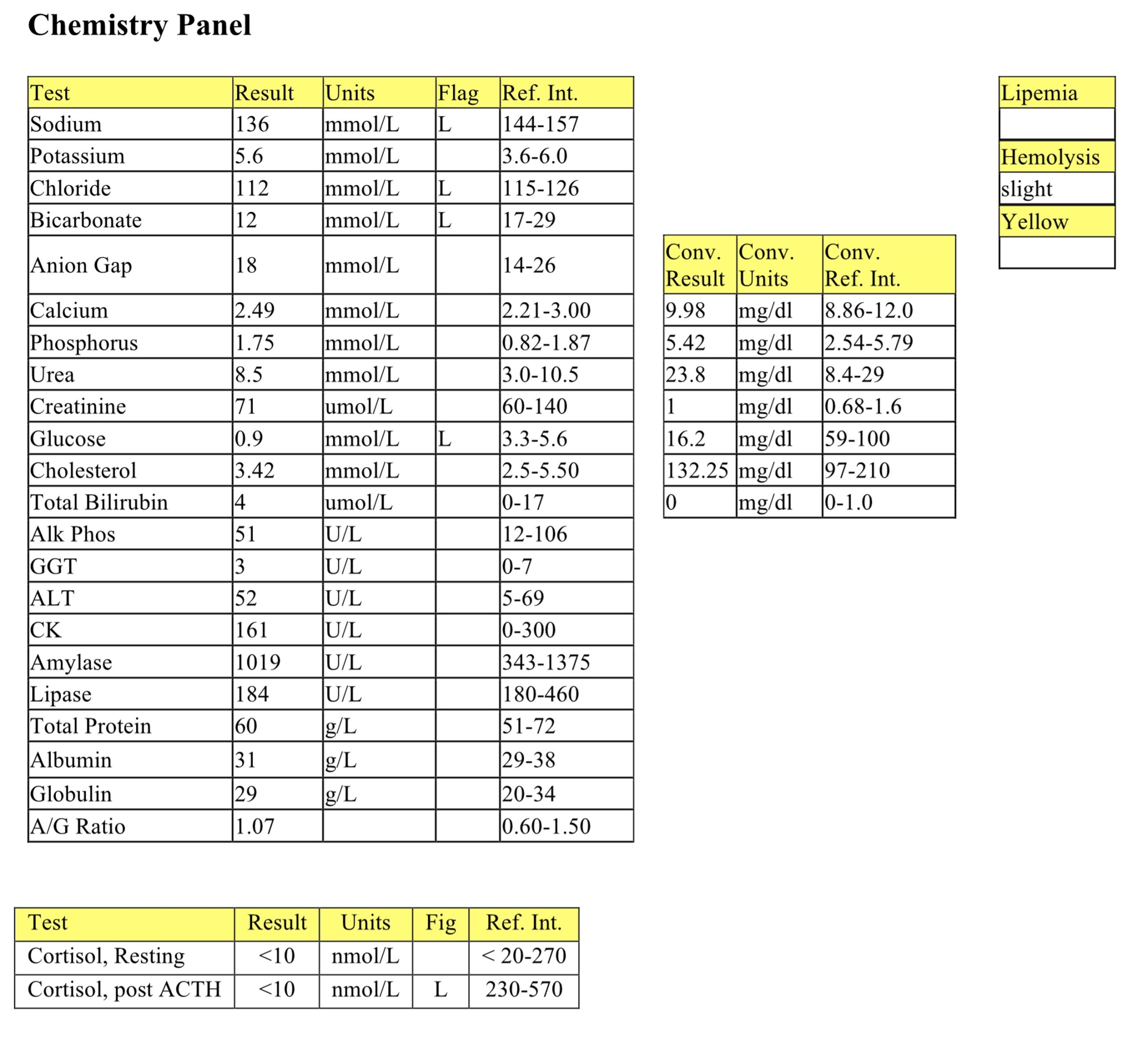
Biochemical Panel
The mild to moderate hyponatremia and mild hypochloremia could be due to increased losses, solute loss in excess of water loss, and/or decreased intake. Lack of mineralocorticoid production results in Na and Cl losses in the urine and K retention. Sodium to potassium ratios of <23:1 are suggestive of, but not diagnostic for, hypoadrenocorticism. The ratio is 24:1 in Thor’s case. The low bicarbonate with a normal anion gap indicates metabolic acidosis due to bicarbonate loss, likely through the kidneys and/or gastrointestinal tract. Marked hypoglycemia can be seen with hyperinsulinism, hepatic dysfunction, sepsis, glucocorticoid lack, and in vitro glycolysis. In this case, sample handling was ruled out, as were other differentials except for glucocorticoid lack. Glucocorticoid lack as well as mineralocorticoid lack usually occur with hypoadrenocorticism.
ACTH Stimulation Test
The baseline cortisol is low normal and there is no response to ACTH. These results are consistent with a diagnosis of hypoadrenocorticism.
Thor most likely has primary hypoadrenocorticism (bilateral adrenocortical destruction) as the CBC supports glucocorticoid lack and the biochemical panel supports both mineralocorticoid and glucocorticoid lack. Animals with secondary hypoadrenocorticism (decreased pituitary ACTH release) will not have electrolyte disturbances as mineralocorticoid production is not affected. Other potential indicators of hypoadrenocorticism are: hypercalcemia, isosthenuria/azotemia, hypoalbuminemia, nonregenerative anemia, and lack of stress eosinopenia and monocytosis. Note that Thor did demonstrate a lack of stress eosinopenia and monocytosis, but these were subtle findings. The major support for the diagnosis in Thor’s case was the lack of neutrophilia and lymphopenia in a stressed/ill patient, hypoglycemia, hyponatremia, hypochloremia, and lack of increase in cortisol in response to ACTH.
-
Wally
CBC
The erythrogram is unremarkable. The mild elevation in RDW is unlikely to be clinically significant, but may correspond to anisocytosis at 2+. Nuclear remnants and Heinz bodies are not unusual to see in low numbers in feline blood as the feline spleen does not efficiently remove such structures from the blood. Rouleaux, at 1+ is also not unusual for feline blood. While mild neutrophilia and lymphopenia represent a stress leukogram, concurrent mild inflammation cannot be ruled out. Giant platelets are also commonly seen in feline blood; however they can also be seen with increased platelet turnover.
Biochemical Panel
The very mild hypercalcemia may relate to increased protein binding as volume contraction is likely (high normal total protein and mildly increased globulins). The mild elevation in urea can be associated with volume contraction (prerenal azotemia), renal azotemia, ingestion of a high protein diet, or intestinal bleeding. Creatinine may not be concurrently elevated with azotemia, if there has been significant loss of muscle mass. The mild hyperglycemia is consistent with stress. Very mild hypercholesterolemia is not considered to be significant. The mild to moderate elevation of ALT activity can originate either from liver or muscle – given the history and CK elevation, as well as lack of changes in other hepatic enzyme activities, the ALT origin is likely muscle. The marked elevation of CK activity indicates severe muscle injury. Mildly elevated lipase activity is likely not significant in context with the clinical and laboratory findings, and may originate from a non-pancreatic source. The mild hyperglobulinemia is most likely a result of volume contraction (both total protein and albumin levels are high normal).
The history, stress leukogram, and evidence of severe muscle injury and volume contraction are highly suggestive of aortic thromboembolism in this patient. Urinalysis is recommended to determine if there is concurrent renal damage or whether the azotemia is prerenal. Imaging of the heart and T4 evaluation would also be recommended to determine if cardiac pathology is a predisposing factor and also to determine if hyperthyroidism is a predisposing factor, respectively. However, it is very likely that this patient would have a low T4 concentration due to severe concurrent illness. Under such circumstances, it is better to stabilize the patient (if possible) and determine the T4 when the patient is feeling better.
-
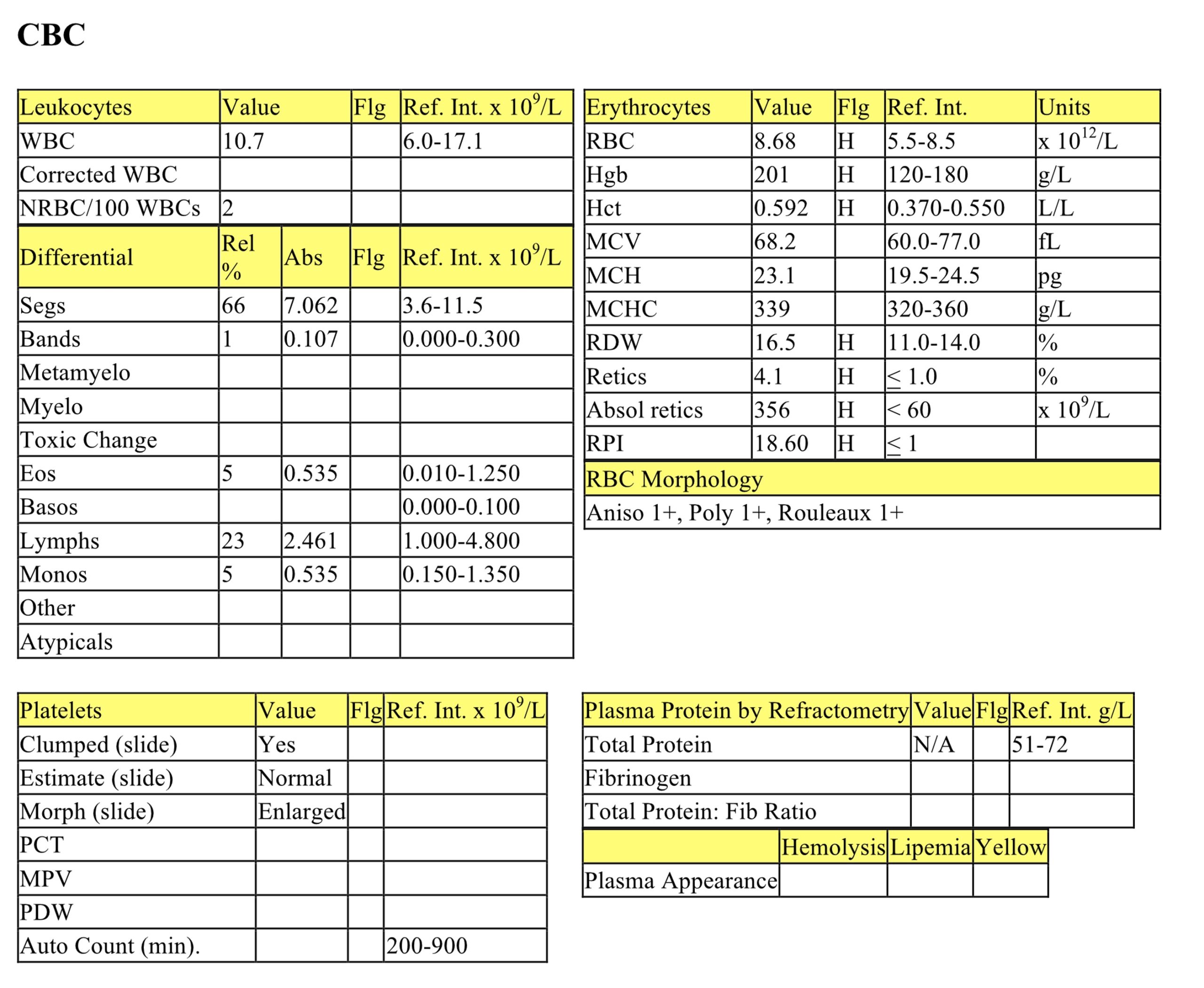
Ronaldo
CBC
Ronaldo has a mild erythrocytosis characterized by elevated Hct, Hgb, and RBC count. Along with the erythrocytosis there is a moderate regenerative response based on reticulocyte percent and absolute count, RPI, and presence of polychromasia. The erythrocytosis may be relative: water excretion may exceed water intake in PU/PD animals, resulting in dehydration. The mild elevation in total protein (see chemistry panel) provides additional support for dehydration. However, there is also a regenerative response possibly due to recovery from prior anemia from blood loss or hemolysis. Absolute erythrocytosis as may occur with chronic cardiac and/or pulmonary disease should also be considered and this could explain a regenerative response in the presence of a normal or elevated Hct. Mildly elevated RDW suggests an increase in variation in erythrocyte size; however, this is not reflected in the degree of anisocytosis noted on smear evaluation. The leukogram is unremarkable and does not reflect stress; however, this patient may not be particularly ill/stressed.
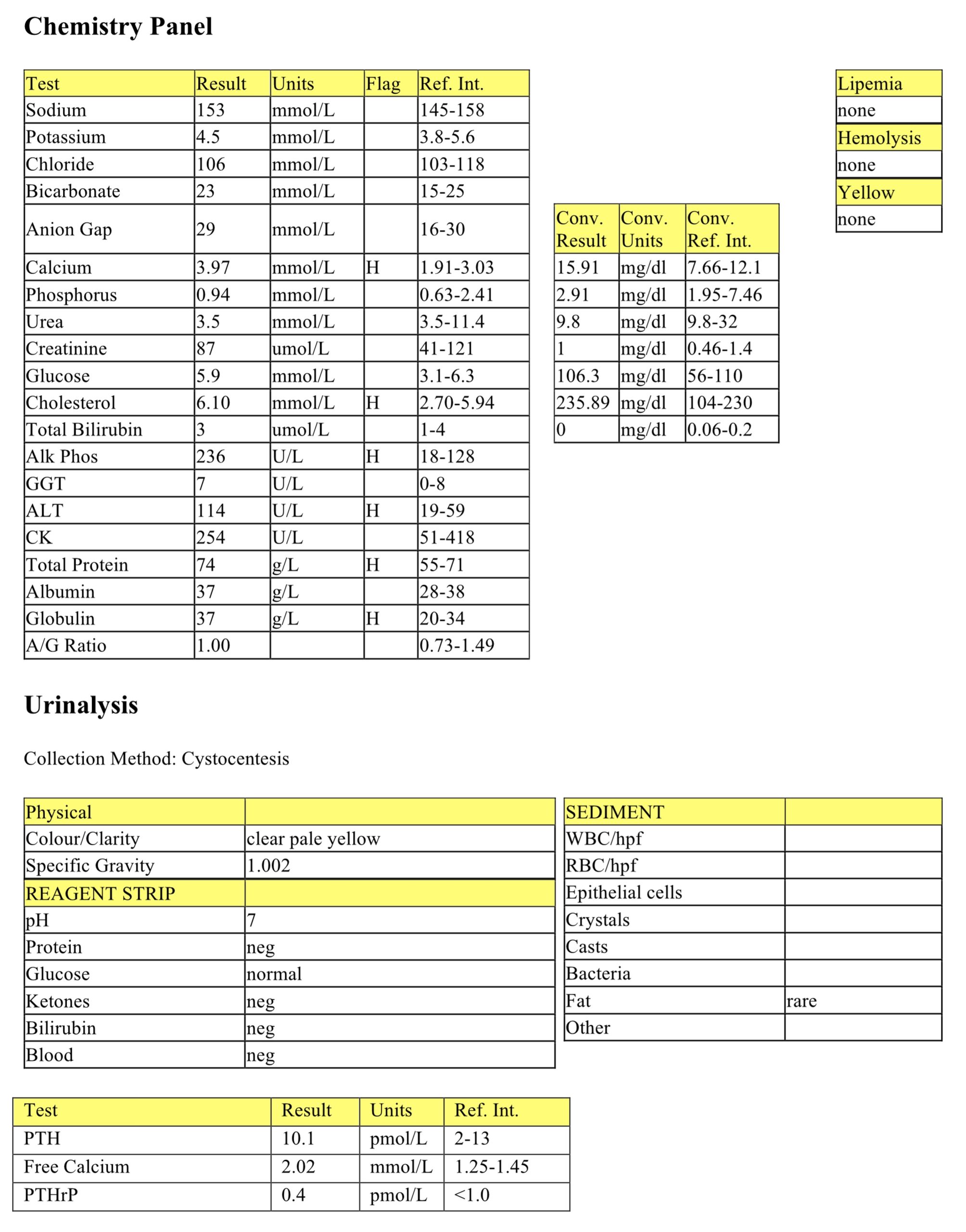
Biochemical Panel
Moderate hypercalcemia is noted and later confirmed to represent an increase in free calcium. Excess PTH will promote calcium release through bone resorption and phosphorus excretion through the kidneys. Usually one would see a drop in serum phosphorus concentration in hyperparathyroid cases; Ronaldo’s phosphorus concentration is low normal and may be slow to decline. The hypercalcemia in turn is likely responsible for Ronaldo’s PU/PD symptoms as calcium has an antagonistic effect on antidiuretic hormone at the level of the renal tubules, promoting fluid excretion. The mild hypercholesterolemia is not likely significant and is probably a result of postprandial sampling. Mild elevation in ALP activity can be a result of enzyme induction, cholestasis, or from a bone source. Mild elevation in ALT activity is likely hepatic origin: elevation can be associated with age-related hepatic nodular hyperplasia in older dogs. The mild hyperproteinemia, high normal albumin, and hyperglobulinemia are most likely a result of dehydration.
Urinalysis
The USG indicates Ronaldo’s urine is markedly dilute (hyposthenuric) which indicates her kidneys are functioning normally in light of her PU/PD history. Renal disease would be indicated by isosthenuria (USG 1.008-1.012) and azotemia which Ronaldo does not have. Otherwise, the urinalysis is unremarkable. The reason for the hyposthenuria, as indicated earlier, is likely hypercalcemia.
PTH and PTHrP
Free calcium, the active form, is moderately elevated. Despite the hypercalcemia, PTH concentration is high normal. Normally when free calcium concentration is high one would expect PTH to be low normal or lower than the RI to maintain calcium homeostasis. The high normal PTH and elevated free calcium concentrations are highly indicative of primary hyperparathyroidism. The low PTHrP concentration rules out production of a PTH-like protein as a cause of hypercalcemia. Elevated PTHrP concentration may be seen as a paraneoplastic cause of hypercalcemia with tumors such as lymphosarcoma and apocrine gland adenocarcinoma of the anal sac.
-
Dan
CBC
The moderate erythrocytosis is likely relative due to Dan’s history of watery diarrhea and clinical evidence of dehydration. The mild increase in RDW suggests increased variation in erythrocyte size. The leukogram indicates Dan has a mild inflammatory response characterized by very mild neutrophilia, mild left shift, and a mild monocytosis. The mild lymphopenia indicates concurrent stress. The absolute hyperfibrinogenemia provides additional support for inflammation. Despite the inflammation and dehydration, a mild decrease in total plasma protein is reported on refractometry. It should be noted that equine vasculature becomes quite “leaky” during bouts of diarrhea which can result in significant protein loss through the intestinal tract. Therefore a low total protein can be expected in cases of equine diarrhea and dehydration is masked by the protein losses.
Biochemical Panel
The electrolyte disturbances seen on the biochemical panel are typical for diarrhea cases. The mild hyponatremia, hypokalemia, and hypochloremia can be associated with loss through the intestinal tract coupled with lack of intake. Mild hypocalcemia may relate to decreased protein binding, given the hypoalbuminemia. Azotemia is noted and characterized by moderate elevations in phosphorus and urea and mild elevation in creatinine, again most likely due to dehydration. However, urinalysis would be required to differentiate between prerenal and renal azotemia. The disproportionate increase in urea relative to creatinine could also be explained by intestinal blood loss, decreased muscle mass, or both. Mild elevation in SDH activity indicates mild hepatocellular damage has occurred, possibly due to poor liver perfusion. Mild elevation in CK activity is likely due to handling or venipuncture. There is a mild hypoproteinemia characterized by a mild hypoalbuminemia and low normal globulin levels. As stated earlier, horses with diarrhea may lose additional proteins due to leaky vasculature in response to inflammation. The globulin loss is likely masked by inflammation (increased acute phase proteins) and/or antigen stimulation as Dan has been ill for several days. In addition to albumin loss through the diarrhea, synthesis may be decreased through its role as a negative acute phase protein.
Dan may be a candidate for an enteric bacterial infection. Bacterial culture of the feces would be recommended. Close monitoring of the CBC would also be recommended as rapid deterioration could occur.
-
Zack
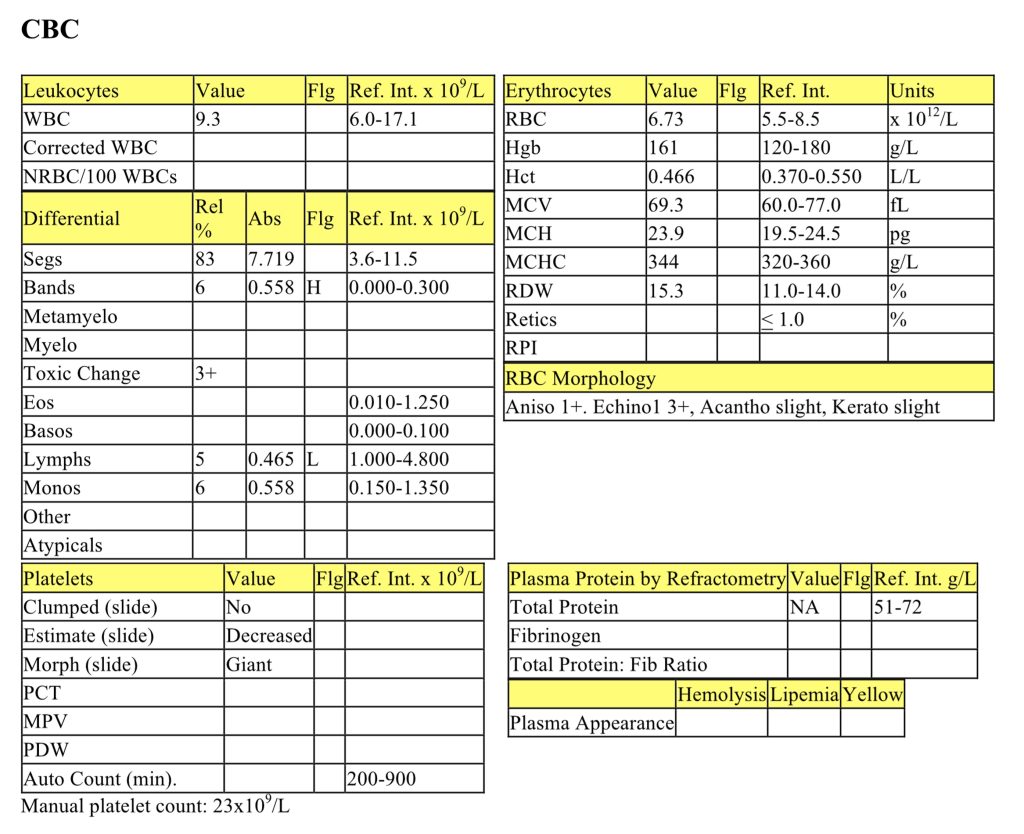
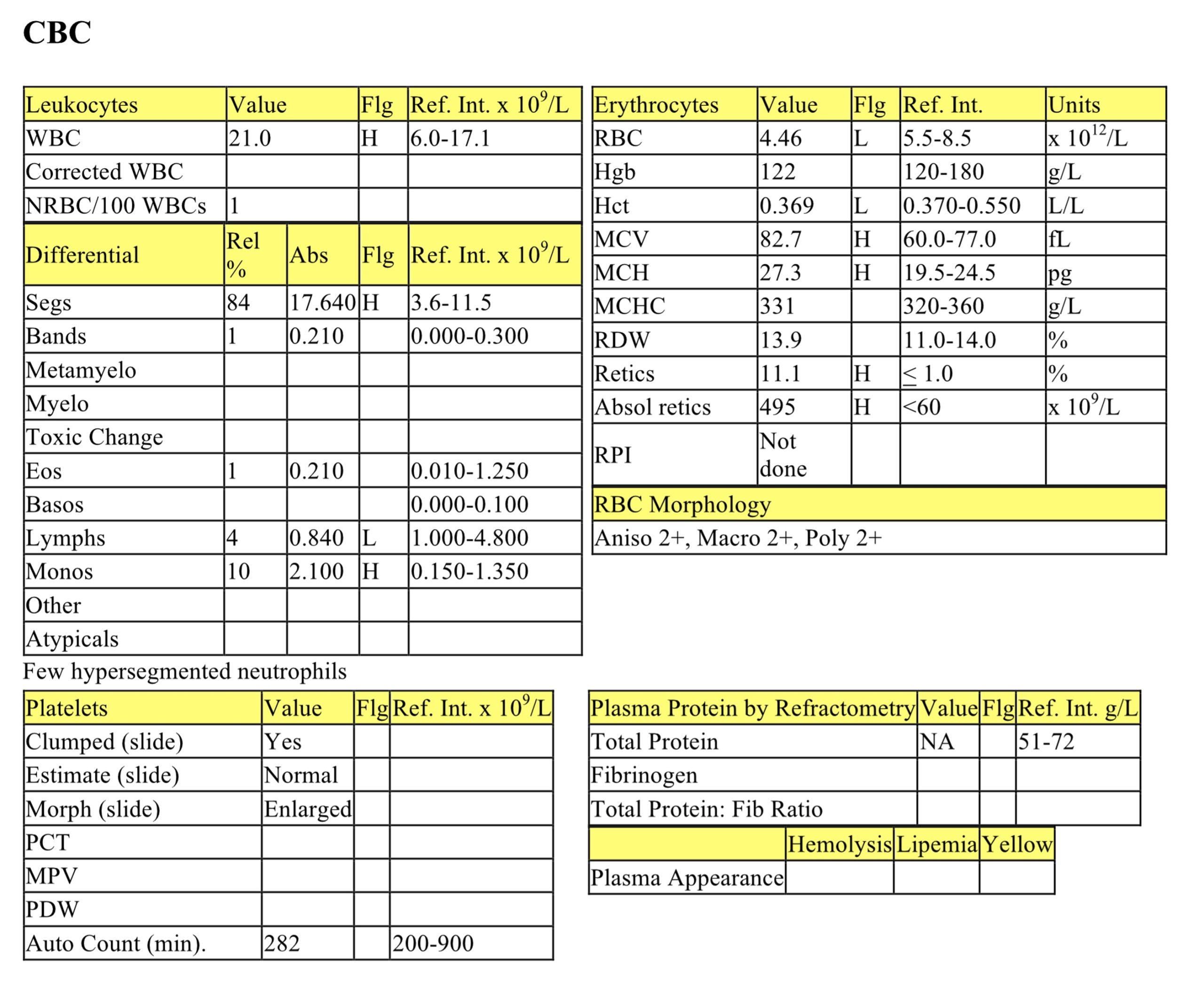
CBC
The erythrogram is unremarkable except for the presence of slight keratocytes and acanthocytes. Keratocytes are formed from mechanical shearing, usually due to fibrin deposition. Acanthocytes may be an incidental finding or they may be seen with hemangiosarcoma, hepatic disease, disorders of lipid metabolism or as a consequence of a high fat diet. The mild left shift with marked toxic change suggests acute and severe inflammation. Moderate lymphopenia is consistent with stress. Zack has a marked thrombocytopenia. Although immune mediated destruction of platelets cannot be ruled out, DIC&F is more likely the cause of the thrombocytopenia because of the clinical presentation and the degree of toxic change associated with the inflammatory leukogram.
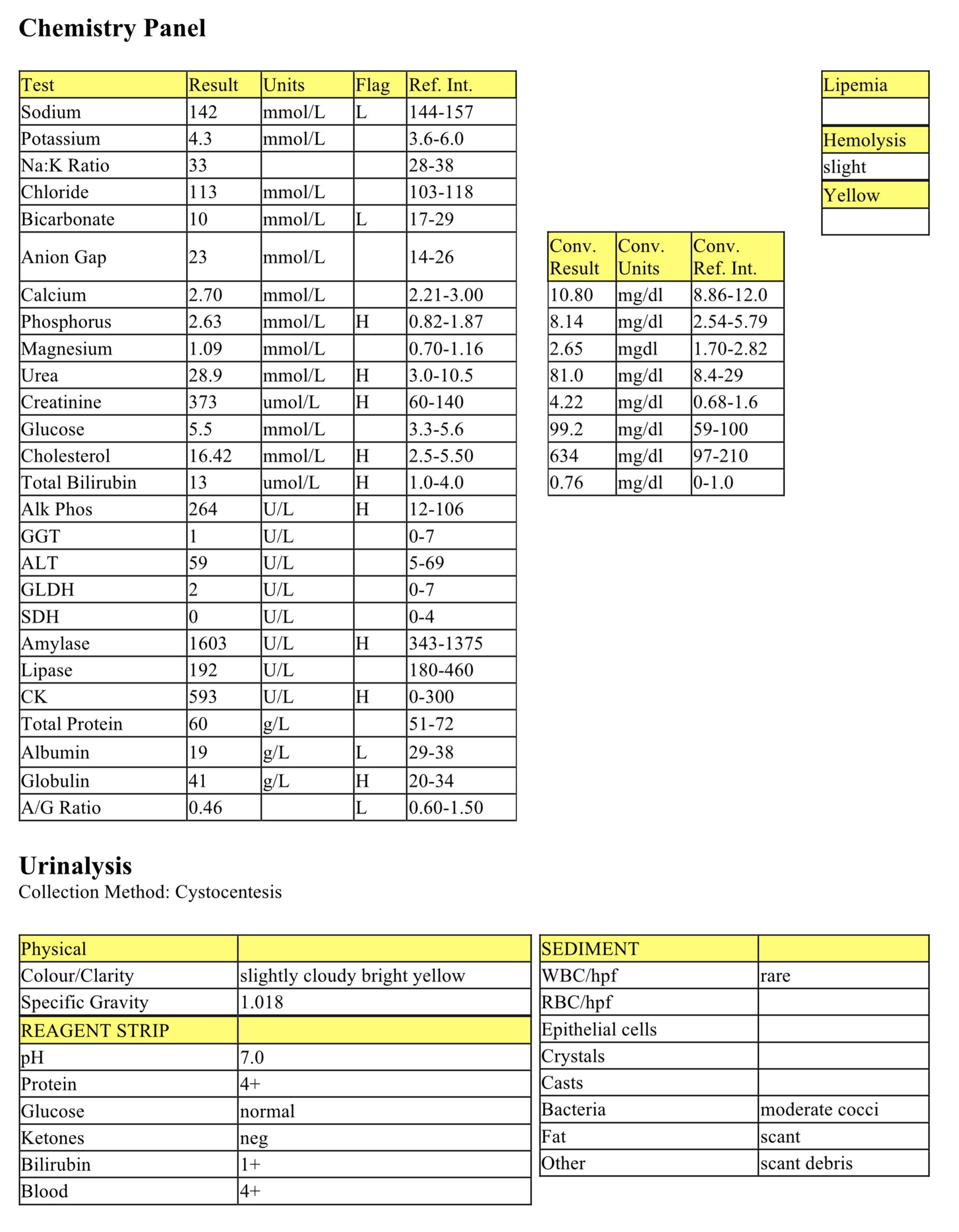
Biochemical Panel
The mild hyponatremia may be due to hemorrhage/GIT loss although decreased intake may also be a contributing factor. Moderate decrease in bicarbonate, high normal chloride, and a normal anion gap suggests a secretory metabolic acidosis usually due to intestinal or renal loss of bicarbonate. The mild hyperphosphatemia is likely due to decreased GFR. The elevated concentrations of urea and creatinine indicate renal azotemia given the USG (see interpretation below). The moderate hypercholesterolemia, hyperbilirubinemia and elevation of ALP activity strongly indicate cholestasis. Mild elevation in amylase activity is likely due to decreased GFR and not particularly significant in the context of this case due to the magnitude of its elevation. Mild elevation in CK activity is most likely due to venipuncture and/or handling. The moderate hypoalbuminemia and mild hyperglobulinemia are consistent with inflammation due to downregulation of negative acute phase protein synthesis (albumin) and upregulation of positive phase protein synthesis (globulins). Hypoalbuminemia can also be associated with renal loss while hyperglobulinemia can be due to chronic antigen stimulation or neoplastic processes.
Urinalysis
Although not isosthenuric, the USG indicates a lack of urine concentration suggesting the azotemia is renal. However, it is unknown if Zack received intravenous fluids prior to collection of the urine sample which could have resulted in lowering of the USG. If fluids were administered prior to urine collection, we cannot be certain if the azotemia is renal or prerenal. There are no intact RBCs to explain the 4+ blood, therefore hemoglobin due to lysed RBCs or myoglobin need to be considered. The significance of the bacterial presence cannot be determined as the sediment is quiet (i.e. no inflammation/pyuria), and a urine culture is recommended. 4+ protein in a non-concentrated urine may be significant, however a UPC is required to further evaluate.
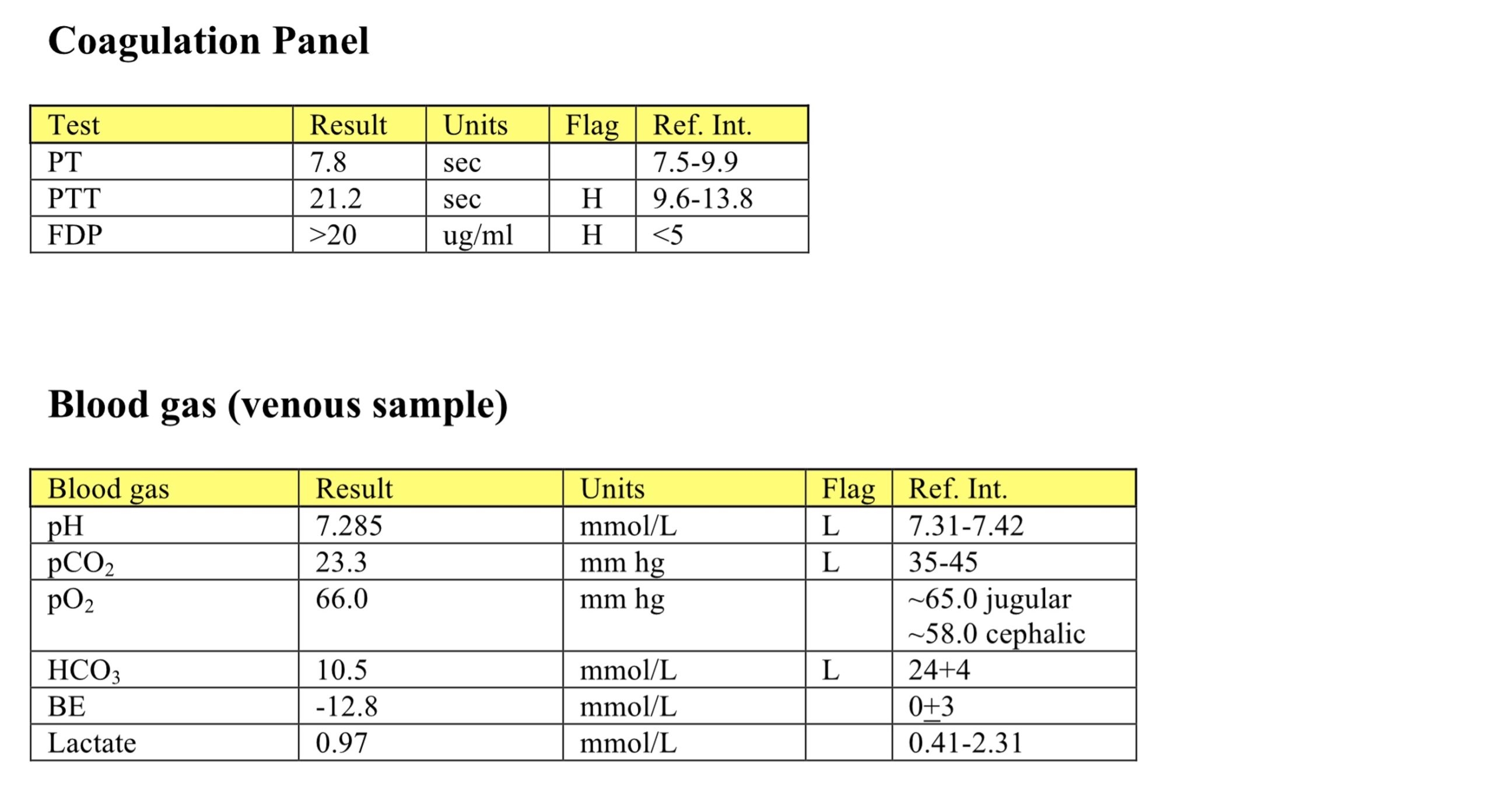
Coagulation Panel
Prolonged PTT and marked elevation of FDPs support DIC&F.
Blood Gas Panel
The low pH and moderate decrease in HCO3 are consistent with the secretory metabolic acidosis described in the biochemical panel. Blood lactate is within the RI indicating that the metabolic acidosis is not due to accumulation of lactate. This finding is consistent with the normal anion gap on the biochemical panel indicating that there is no evidence of acid gain. The decreased pCO2 is an appropriate respiratory compensation response as Zack would be hyperventilating in an attempt to eliminate the excess acid in his body.
Overall Zack likely has DIC&F based on the finding of thrombocytopenia, keratocytes, as well as the prolonged PTT and elevation of FDP concentration. DIC&F is always secondary to another disease process, in this case likely an inflammatory process. With the marked toxic change and acute inflammatory response, blood culture is recommended.
Follow up: due to the severity of his condition, Zack was euthanized and his body was submitted for a complete necropsy. Bacterial culture isolated 4+ Streptococcus canis from the kidney, lung and left atrioventricular valve, and there were bacterial emboli found in all tissues indicating septicemia was the most likely cause for the DIC&F. Also Zack had renal agenesis as he had no right kidney. His left kidney was noticeably larger and histopathology confirmed acute severe embolic (bacterial) nephritis as well as chronic renal disease. Zack’s left ventricular myocardium also had areas of necrosis with neutrophils and bacterial emboli. The final diagnosis made was septicemia, renal agenesis, acute embolic nephritis, chronic renal failure, meningitis, valvular endocarditis, thrombosis, myocarditis, and diffuse pericarditis.
-
Sauron
CBC
The erythrogram indicates mild anemia based on low normal to slightly decreased Hct, Hgb, and RBC values which can be attributed to prior hemolysis as indicated in the history. There is a marked regenerative process characterized by marked reticulocytosis, polychromasia, increased MCV and macrocytosis. The mild elevation in MCH can be attributed to the regenerative response (larger RBCs with more hemoglobin content). Lack of spherocytes, agglutination, Heinz bodies, eccentrocytes, and RBC parasites helped to rule out more common causes of hemolytic anemia in dogs. The mild leukocytosis is characterized by a mild neutrophilia and mild monocytosis, along with a mild lymphopenia. These findings could be entirely due to stress/steroid influence, however, concurrent inflammation cannot be ruled out. High doses of exogenous steroids may be responsible for the “classic” stress leukogram in this patient, rather than lymphopenia alone.
Biochemical Panel
Mild hyperbilirubinemia is likely associated with prior/ongoing extravascular hemolysis, given the history and CBC findings. Elevation of SDH activity indicates hepatocellular injury, however this elevation is very mild and unlikely to be clinically significant. Mild elevation in CK activity is likely due to venipuncture and/or handling. There is a mild elevation in the A/G ratio due to both mildly elevated albumin and low normal globulins. The albumin concentration could be normal for this patient; however, mild dehydration may also be present. Lack of antigenic stimulation could explain the globulin concentration.
Urinalysis
The UA results indicate the presence of urinary tract inflammation and infection as there is mild pyuria in the sediment along with the abundance of bacterial rods. Corticosteroid treatment may have predisposed this patient to the UTI. Although bilirubinuria can be seen in normal dogs, in this case its presence could reflect hyperbilirubinemia. Recommended tests include urine culture and sensitivity.
As Sauron is a young English Spaniel dog with a history of recurrent hemolysis and pigmenturia, he is an ideal candidate to suspect phosphofructokinase (PFK) deficiency – a disease first recognized in English and American Cocker Spaniel dogs. PFK is an enzyme involved in ATP and 2,3-BPG formation. Deficiencies lead to decreased ATP production and ultimately impaired erythrocyte function and premature destruction. Decreased 2,3 BPG production leads to increased erythrocyte alkaline fragility. PFK deficient animals will often have a mild to moderate anemia accompanied by a disproportionately high reticulocyte response. Although not mentioned in Sauron’s history, these animals often have periods of collapse or pigmenturia after episodes of excitement, exercise, prolonged barking, or any other activity involving hyperventilation and transient respiratory alkalosis. Genetic testing is recommended to confirm PFK deficiency.
A PCR test was performed on a blood sample from Sauron and the expected mutation was detected. This condition can be managed in affected dogs by avoiding strenuous exercise, overheating, panting, and excessive barking.
Erythrocyte rupture or destruction; may occur in vitro or in vivo as a pathologic process.
Increased number of erythrocytes with decreased volume that usually corresponds with decreased MCV; often associated with iron deficiency as well as portosystemic shunts.
Decrease in hematocrit (PCV) recognized on the complete blood count (CBC); usually hemoglobin concentration and RBC numbers are also decreased.
Anemia due to destruction of RBCs. Lysis may be intravascular (within blood vessels) or extravascular (within tissues rich in mononuclear phagocytes such as spleen and liver), or both.
All tests on the complete blood count (CBC) that evaluate erythrocytes, including morphologic examination on the peripheral blood smear.
Variation in cell size.
Increase in the number of neutrophils in peripheral blood.
Release of less mature neutrophil stages (bands, metamyelocytes, myelocytes) from the marrow into the peripheral blood in response to inflammation.
Increase in the number of monocytes in peripheral blood.
All tests on the CBC that evaluate leukocytes. Also, that part of the leukon which is evaluated by examination of a peripheral blood sample (typically does not include leukocyte precursors).
Mononuclear, non-phagocytic leukocyte responsible for humoral (B lymphocyte) and cell-mediated (T lymphocyte) immune responses.
Mononuclear phagocyte found in tissues that develops from circulating blood monocytes and fulfills many roles in normal immune function including antigen presentation.
Impaired bile flow.
Decrease in the number of neutrophils in peripheral blood below the reference interval for the species.
Granulocyte with large, round, pink to orange (eosinophilic) cytoplasmic granules and an often bi-lobed nucleus; important in host response to allergens and defense against parasites.
Also called Addison’s disease; endocrine disease of dogs associated with decreased production of mineralocorticoids, glucocorticoids, or both due to adrenocortical pathology.
Difference between unmeasured anion and cation concentrations, calculated using the formula: (Na+ + K+) minus (Cl- + HCO3-.)
Urine specific gravity between 1.008 and 1.012, reflecting urine that has been neither diluted nor concentrated by the kidneys.
Increases serum urea and/or creatinine.
Decrease in the number of eosinophils in peripheral blood. May not be detectable given the reference intervals.
Piece of the nucleus that persists in the mature erythrocyte. May be seen in healthy animals, especially cats, and those with regenerative anemias, or hypofunctioning spleens.
“Stack” of red blood cells resembling a roll of coins; prominent in equine and often feline blood. Formation increases as negative charges between RBCs decrease (e.g. with increased plasma proteins).
Typical change seen in peripheral blood of an ill or stressed animal (with increased cortisol levels), consisting of lymphopenia which may be accompanied by neutrophilia and monocytosis (species differences exist).
An anucleate (in mammalian species) cytoplasmic fragment arising from a megakaryocyte; vital for primary hemostasis.
Azotemia due to extracellular fluid volume depletion (dehydration).
Azotemia due to renal disease.
Most abundant plasma protein in health; maintains oncotic pressure.
Common endocrine disease of older cats associated with thyroid gland hyperplasia or a functioning thyroid adenoma.
Increase in hematocrit (PCV) in peripheral blood; usually accompanied by increases in hemoglobin and RBC numbers.
Number of erythrocytes per liter of whole blood (measured).
Anucleate (in mammalian species), immature erythrocyte containing cytoplasmic RNA and ribosomes which are precipitated by staining with new methylene blue.
Reticulocyte production index; a calculated value designed to determine if the regenerative response is adequate for the degree of anemia. Corrects for the longer life of a young reticulocyte and the relative increase in reticulocytes in the presence of a low hematocrit (anemia). Reported for dogs only.
Increased numbers of anucleate, immature erythrocytes that stain bluish-pink with Romanowsky stains due to the presence of cytoplasmic RNA.
Red blood cell (RBC); an anucleate (in mammalian species) cell containing hemoglobin needed for oxygen transport. Typically shaped like a bi-concave disk.
Calcium that is not bound to proteins in serum and is biologically active.
Cellular proliferation- increased number of normal cells.
Constellation of: retention of metabolic waste products, acid-base and electrolyte disturbances, and compromised urine concentrating ability that develops when the functional mass of the kidneys is reduced by 70% or more; may be acute or chronic.
Urine specific gravity <1.007, reflects dilution of the urine by the kidneys.
Unusual cause of hypercalcemia due to increased PTH release from a functional parathyroid tumor.
Solid malignant lymphoid tumor.
Method of measuring the protein content of a fluid that relies on refraction of light, which is proportional to the quantity of solids in solution.
Crescent-shaped cells that are formed from mechanical shearing (usually due to fibrin strand deposition) of the red cell.
Erythrocyte with little central pallor and several irregular membrane projections.
The end product of coagulation, produced by the conversion of fibrinogen.
General term for fat, including triglycerides, phospholipids, cholesterol.
Cytoplasmic abnormalities seen in neutrophils that have not matured normally in the bone marrow. Abnormalities include retention of primary granules, vacuolation, darker staining due to retention of ribosomes, and deposits of rough endoplasmic reticulum (Döhle bodies).
Decrease in the number of circulating platelets below the reference interval.
Disseminated Intravascular Coagulation & Fibrinolysis; simultaneous disorders of coagulation and fibrinolysis due to generalized derangement of hemostasis.
General term for a decrease in number of any cell line in peripheral blood.
Oxygen-carrying molecule within erythrocytes.
Heme protein responsible for oxygen transport in muscle.
See Secondary hemostasis.
Partial thromboplastin time; diagnostic test used to evaluate the intrinsic and common pathways.
Fibrin/fibrinogen Degradation Products; increased concentration of these products supports a diagnosis of DIC&F.
Average erythrocyte size in femtoliters (measured or calculated PCV or Hct÷RBC).
Increased number of erythrocytes with increased volume that usually corresponds with increased MCV; may be seen in regenerative anemias and can be normal in Poodle dogs.
Average amount of hemoglobin per erythrocyte (calculated: hemoglobin÷RBC count).
Erythrocyte with a spherical rather than biconcave disk shape, which results in a compact cell with a lack of central pallor. Often associated with immune-mediated hemolytic anemia.
Erythrocyte in which the hemoglobin is displaced to one side due to oxidative damage to the lipid membrane.
Erythrocyte destruction within macrophages of the spleen, liver, lymph nodes, and bone marrow; often accompanied by hyperbilirubinemia and bilirubinuria.
Nonspecific term for sublethal or lethal injury to hepatocytes due to various causes, e.g. hypoxia, toxins, infection.
Process that adds base (HCO3-) to the blood or removes acid (H+); blood pH may or may not be increased.
