
Microscopic Evaluation of Urine
Microscopic examination is done on a slide prepared from the sediment. The urine sediment is examined for the presence of white blood cells (WBCs), red blood cells (RBCs), epithelial cells, crystals, casts, bacteria, fat, and miscellaneous contents, such as spermatozoa and fungi. The significance of these findings depends, to a certain extent, on their relative abundance and the method of collection. For example, low numbers of WBCs and RBCs, epithelial cells and extracellular bacteria would not be unusual findings in a sample collected by catheterization. High numbers of calcium carbonate crystals are expected in equine urine. RBCs and WBCs will shrink, or swell and lyse depending on the USG (see Laboratory Manual for further details).
White blood cells
Greater than 5 WBCs per high power field (40 x objective) suggests inflammation of the urinary or urogenital tract. The presence of bacteria along with WBCs supports urinary tract infection. Occasionally bacteriuria is present without WBCs. If contamination of the sample has been ruled out, then conditions such as hyperadrenocorticism, diabetes mellitus, immunosuppression, and/or corticosteroid administration, which can result in an impaired inflammatory response to infection, should be considered. Occasionally, bacterial contamination of samples collected by cystocentesis occurs due to aspiration of intestinal contents during the procedure.
Epithelial cells
Squamous epithelial cells from the genital tract or distal urethra are often present in urine samples. Transitional epithelial cells originating from the more proximal urinary tract may also be seen, particularly in catheterized samples and less commonly in cystocentesis samples. Large clumps of transitional epithelial cells or cellular atypia should signal the possibility of urinary tract neoplasia (transitional cell carcinoma). However, urinary tract infection, particularly if chronic, can result in epithelial cell atypia or dysplasia. Also, neoplasia can predispose to urinary tract inflammation/infection. The history, clinical findings, and additional test results are very useful in differentiating these conditions. Repeat sampling following treatment for urinary tract infection can also be useful. Concentrated cytological preparations (cytospin smears) of the urine sediment are particularly useful to the clinical pathologist for evaluating cell morphology under these circumstances.
Crystals
Crystal formation in urine is dependent on several factors, including concentration and relative proportions of the chemical constituents of the crystals, and urine pH. Crystals can also form after collection of the sample, especially if the sample evaporates, ages, or is refrigerated.
Struvite
Struvite crystals are among the most commonly seen in canine and feline urine. Although struvite crystals can be found under normal circumstances, their formation is promoted by alkaline urine which can result from urinary tract infection with urease-producing bacteria. In cats with lower urinary tract disease, struvite crystalluria and hematuria are often seen in the absence of bacteriuria and WBCs. Struvite urolithiasis is a frequent sequela in intact or neutered male cats, necessitating immediate medical treatment.
Calcium oxalate
Calcium oxalate dihydrate crystals are not unusual in urine from normal cattle and horses as they are derived from the high oxalate content of herbivore diets, but are less common in normal cats and dogs. Increased numbers can be seen with disorders of calcium homeostasis, excess intake of calcium, vitamin D, vitamin C, and diets rich in oxalic acid derivatives (spinach, wheat germ, sweet potatoes, and nuts). Ethylene glycol toxicosis can be associated with the presence of calcium oxalate dihydrate or more significantly monohydrate crystalluria, although the absence of these urine crystals does not rule out the diagnosis. Also, with acute renal failure due to ethylene glycol poisoning, calcium oxalate crystals can be present within renal tubules without being passed in the urine.
Calcium carbonate
Calcium carbonate crystalluria is expected in normal horses with hay as a significant portion of their diets. These crystals are also common in the urine of normal rabbits, guinea pigs and goats. They are rarely observed in feline or canine urine.
Bilirubin
Bilirubin crystalluria is most common in dogs, given the low renal threshold for bilirubin in this species and the ability to conjugate bilirubin in their renal tubules. Bilirubin crystals are uncommonly seen in the urine of other species, and causes of increased bilirubin excretion usually must be explored when they are found.
Ammonium urate
Ammonium urate crystals may be seen in certain breeds of dogs, particularly the Dalmatian, English bulldog, and Black Russian Terrier breeds, due to a hereditary defect in purine metabolism. Ammonium urate crystalluria in other breeds of dogs and other species should alert the clinician to the possibility of portosystemic shunting of blood or hepatic failure, in which there is decreased conversion of ammonia to urea.
Other crystals
Calcium phosphate, silica, cystine, xanthine, and tyrosine urine crystals have all been reported and their presence should be interpreted in relation to species and breed, diet, and drugs administered.
Infectious agents
The presence of bacteria or other infectious agents in the urine should be evaluated in light of the method of collection, history, sample handling procedures, and additional urinalysis findings.
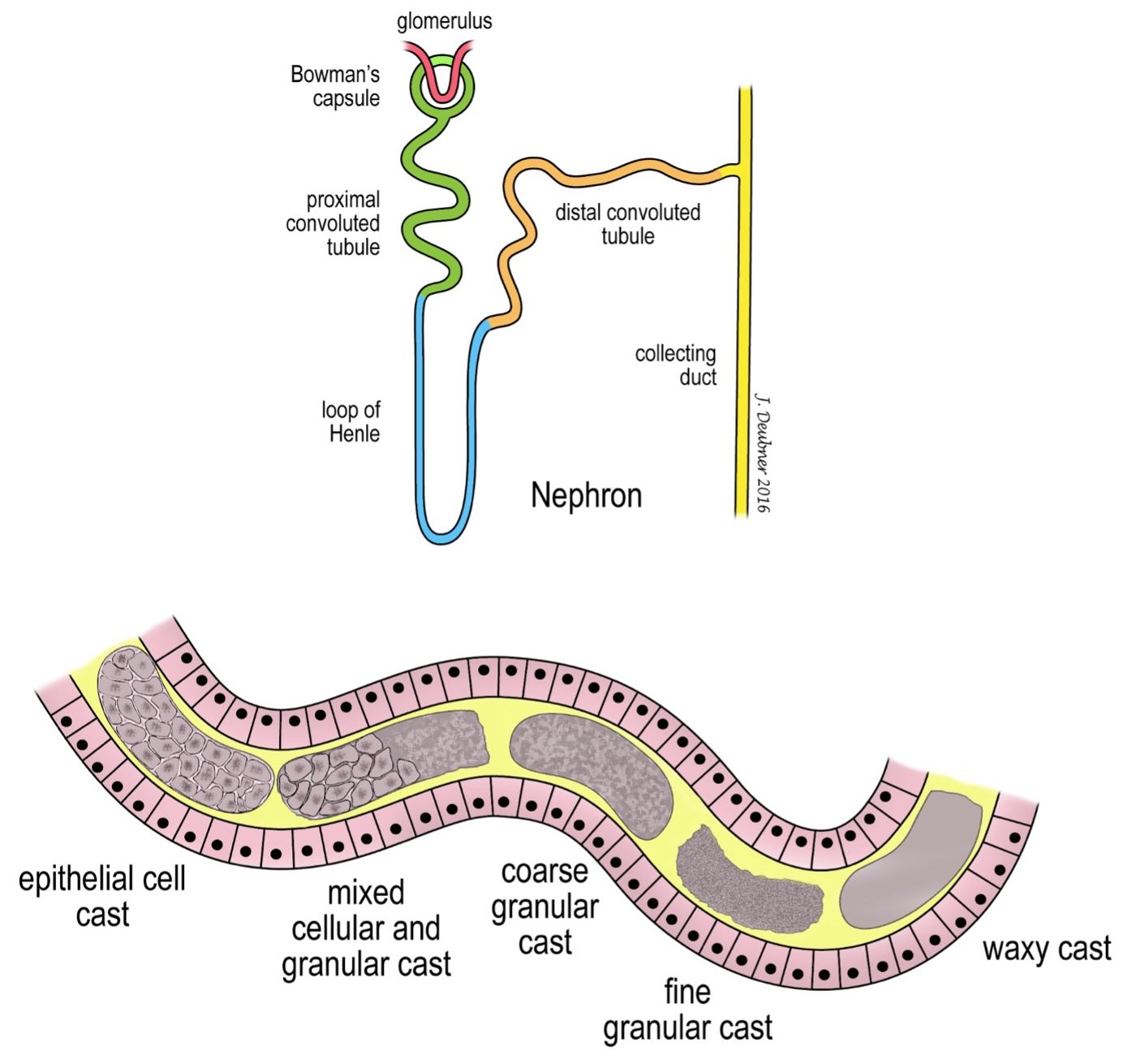
Casts
Urine casts are long cylinders with smooth sides and often irregular ends. They are formed in the renal tubules and comprise one or more of: epithelial cells, leukocytes, protein, necrotic material, and fat. Casts of intact or degenerating epithelial cells indicate tubular injury. As the cells degenerate further, the casts change from coarse and granular to fine and granular, and ultimately, to an amorphous “waxy” appearance (Fig. 7.2). Leukocyte casts suggest renal inflammation, although differentiation between degenerating epithelial cells and leukocytes can be difficult to impossible. Hyaline casts are smooth and acellular, and suggest renal protein loss. Visualization of hyaline casts requires reduced microscope illumination.
Method of urine collection involving insertion of a needle directly into the urinary bladder via the abdominal cavity, bypassing the lower urinary tract.
Malignant neoplasm of epithelial origin, e.g. squamous cell carcinoma.
