
Left Shift and Toxic Change
The release of immature neutrophils, usually bands but sometimes also metamyelocytes and myelocytes, from the bone marrow into the peripheral blood is called a left shift. A left shift can be seen with inflammation of all durations, but is generally more severe with acute, overwhelming inflammation.When the demand for neutrophils is great, transit times in both mitotic and post-mitotic pools may be shortened, such that neutrophil cytoplasms do not mature normally. Cytoplasmic abnormalities associated with the increased rate of neutrophil production are referred to as toxic change and include: retention of primary granules, vacuolation, darker staining due to retention of ribosomes, and deposits of rough endoplasmic reticulum which appear as dark blue irregular granules, called Döhle bodies, with Romanowsky stains (see Fig. 2.3 for normal neutrophil morphology and Fig. 2.4 for toxic change in neutrophils). Toxic change is graded in cells of the neutrophil lineage in the peripheral blood and is often associated with the presence of a left shift. The grading scheme relates to the severity of the cytoplasmic abnormalities as well as the proportion of cells affected. If a patient does not succumb to the acute, overwhelming phase of the inflammatory process, then the bone marrow generally has an opportunity to recover and hyperplasia of the neutrophil lineage may occur. With time, this may be reflected in the CBC as neutrophilia, possibly with a mild left shift and less toxic change. These leukogram changes depend on how quickly and completely the inflammatory process resolves.
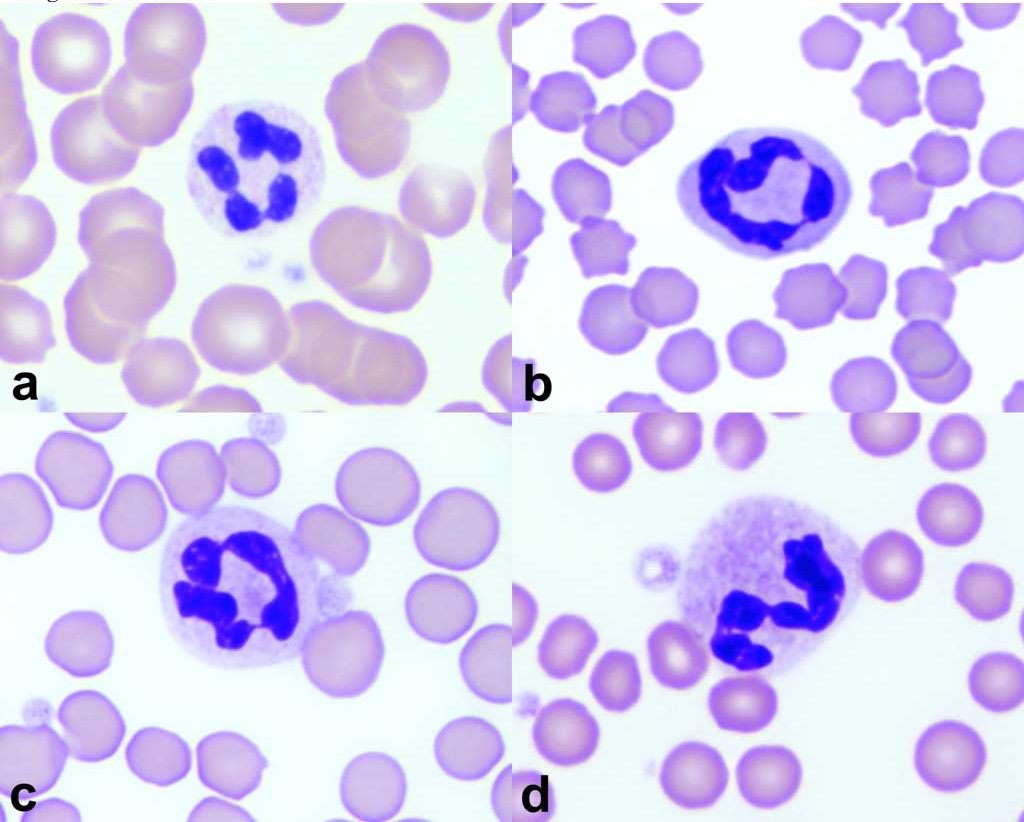
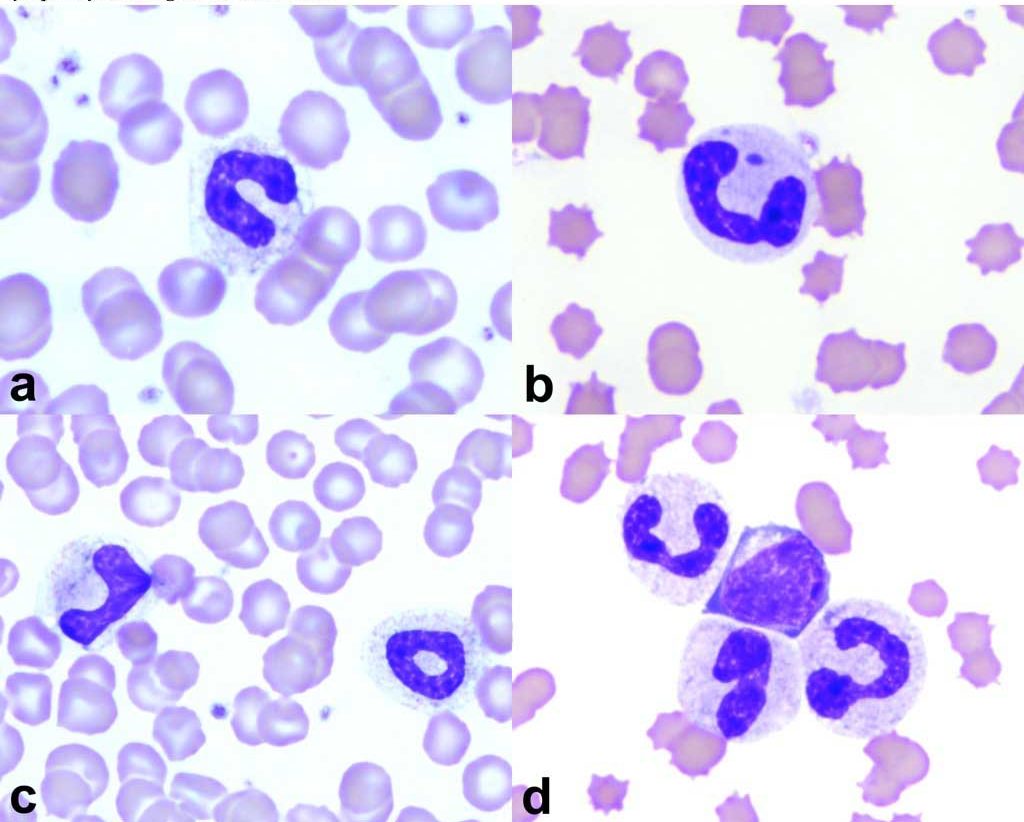
Cytoplasmic abnormalities seen in neutrophils that have not matured normally in the bone marrow. Abnormalities include retention of primary granules, vacuolation, darker staining due to retention of ribosomes, and deposits of rough endoplasmic reticulum (Döhle bodies).
Routine stain for blood smears.
Cellular proliferation- increased number of normal cells.
