
Case Studies
Case 1. Bill
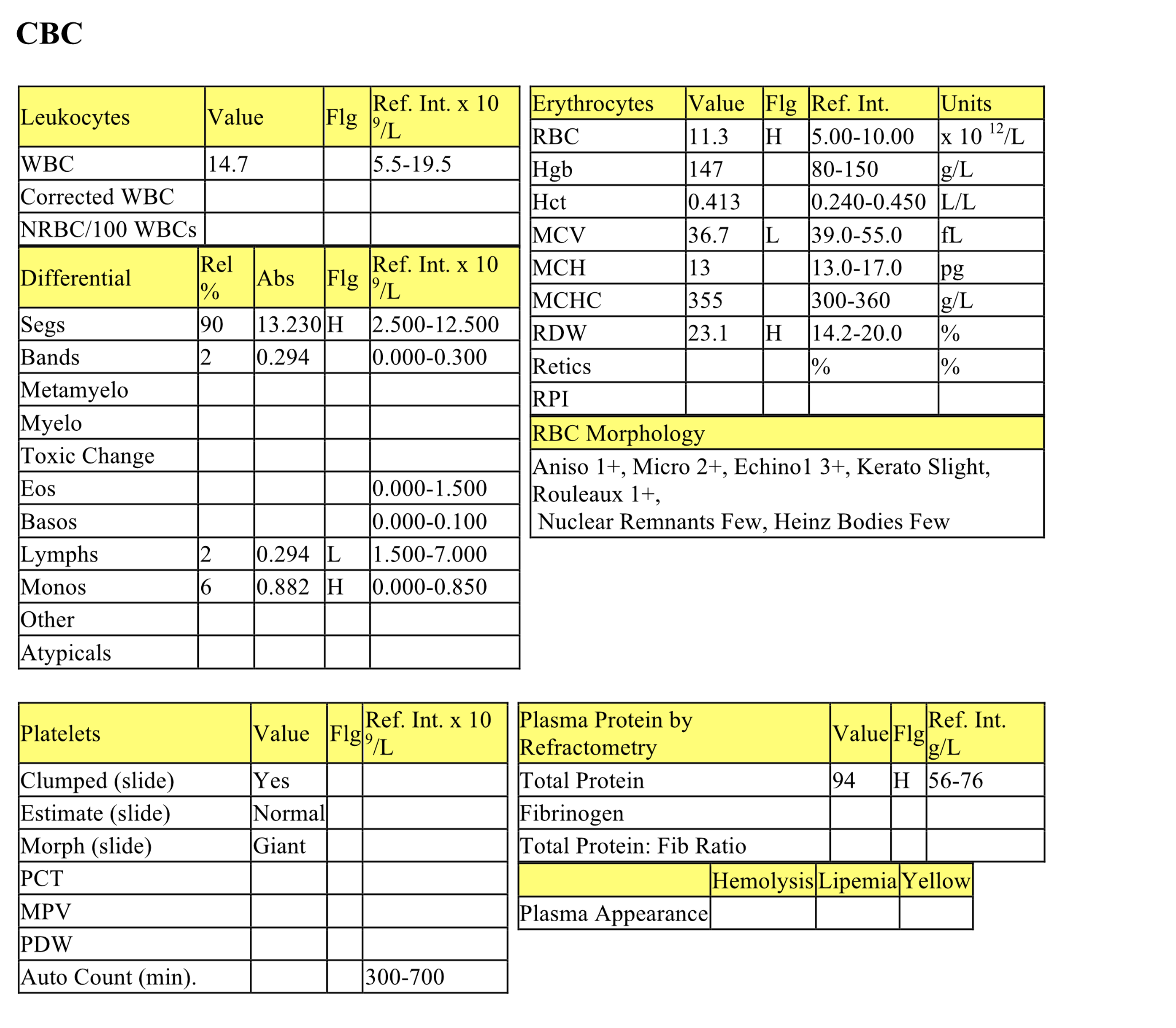
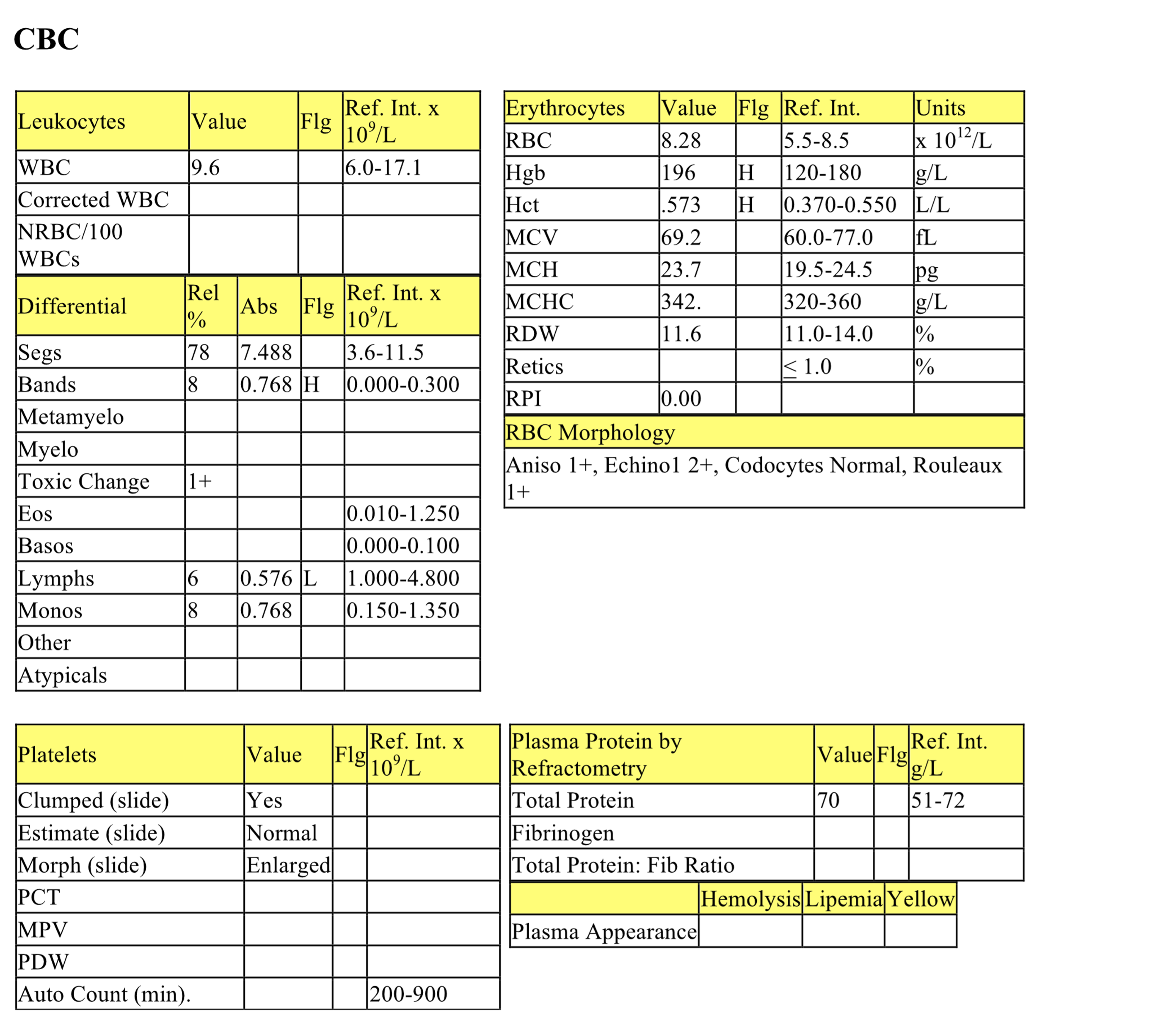
Bill, a 1-year-old M(c) DSH cat, had very recent lethargy, depression, sore mouth, and polydipsia.
CBC
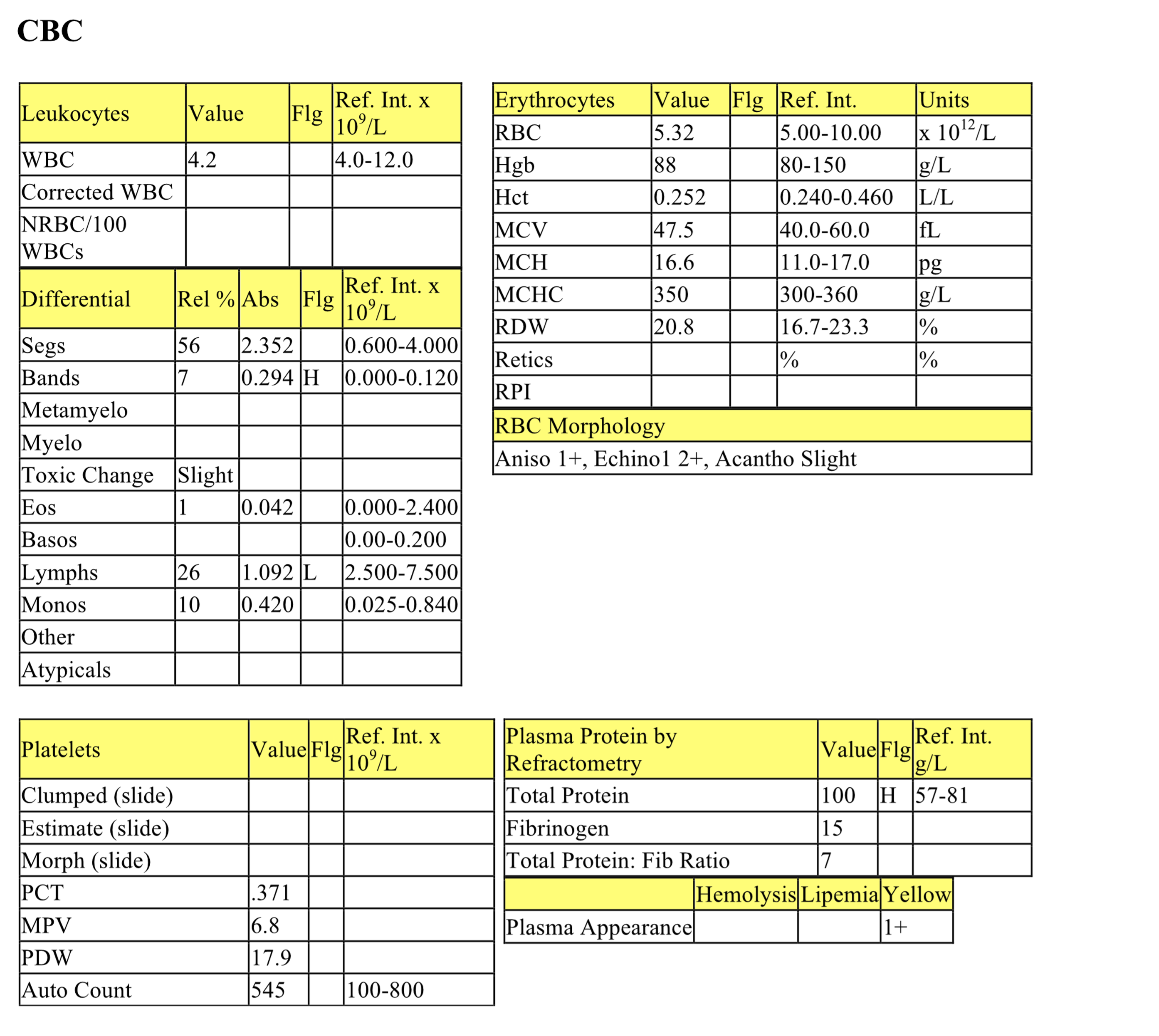
The mildly increased RBC count, high normal hematocrit and hemoglobin concentration, and increased total protein suggest dehydration (which is also supported by the high normal albumin on the biochemical panel). The extreme electrolyte and acid-base changes may be responsible for microcytosis and echinocytosis (reflected in decreased MCV and RBC morphology). Increased RDW reflects the variability in RBC size and generally correlates with the degree of anisocytosis.
Although the WBC count is within the RI, there is a mild neutrophilia, marked lymphopenia and mild monocytosis consistent with a stress leukogram. Bands are high normal, so there may be a developing inflammatory leukogram; however, this degree of band release can also be seen from stress alone. Total protein by refractometry is higher than the protein on the biochemical panel likely due to interference by urea, a substance that can increase the refractive index and therefore the total protein reading. Also, fibrinogen is included in the refractometric reading on the plasma, but is not contained in serum.
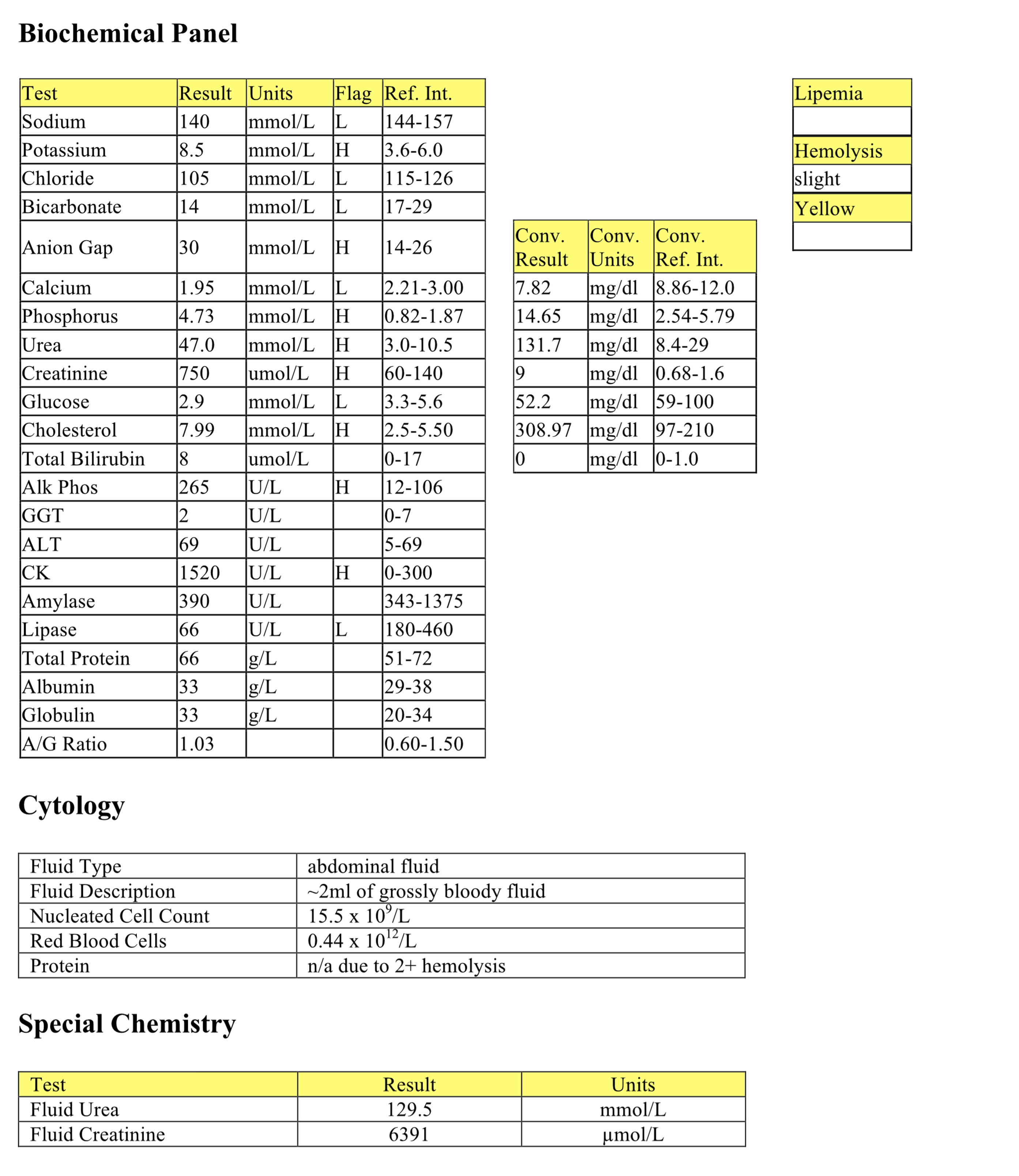
Biochemical Panel
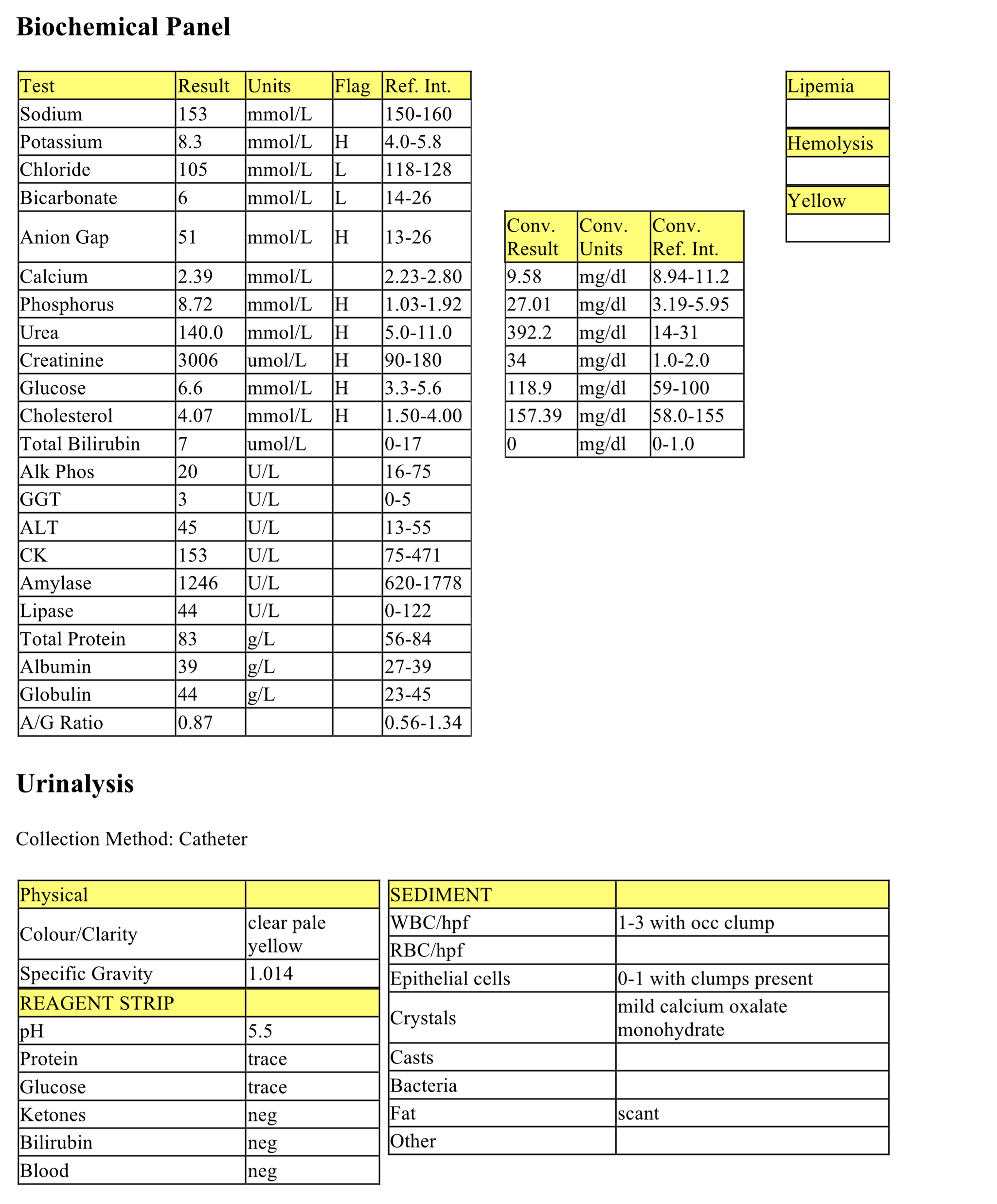
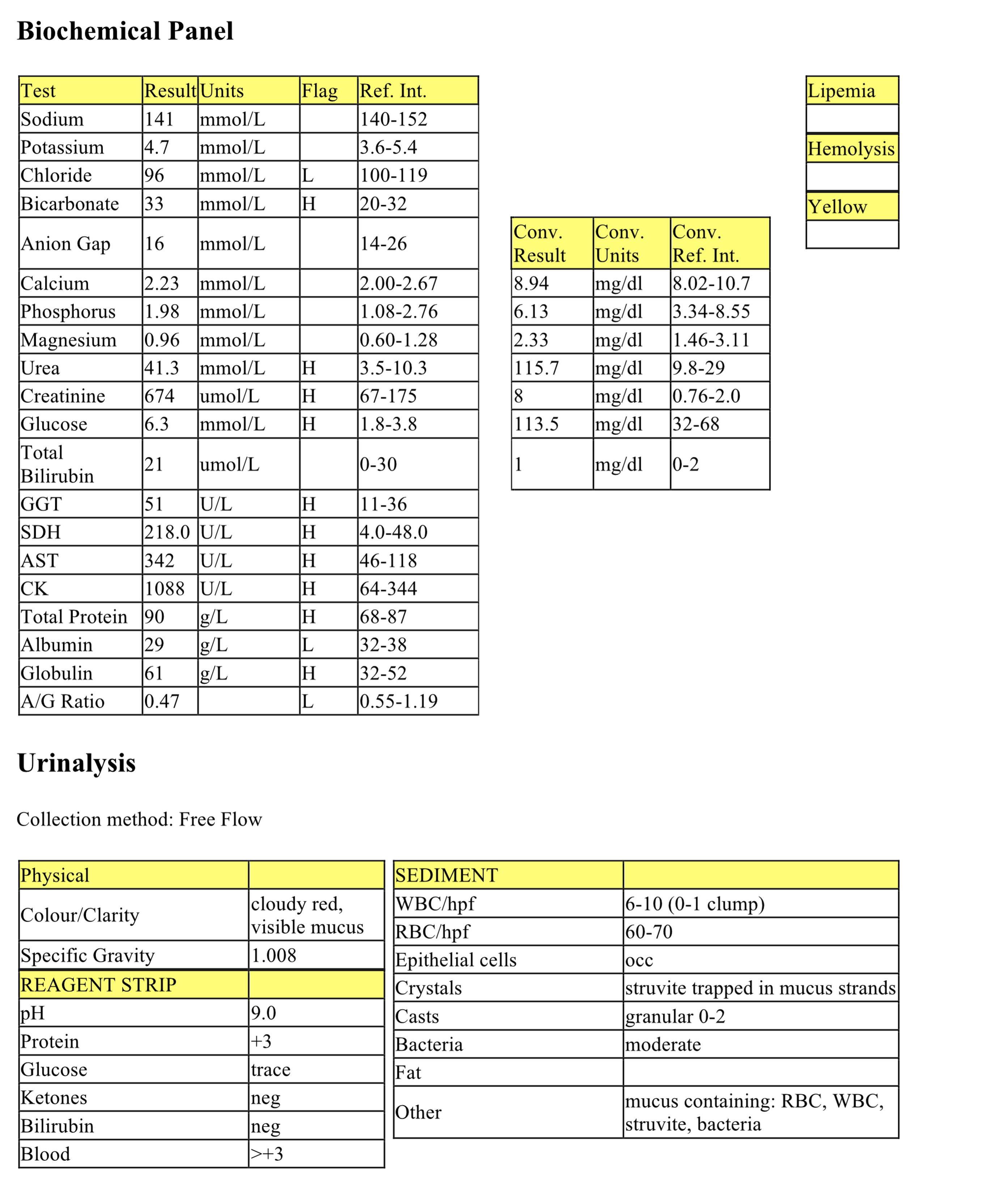
Marked hyperkalemia is likely due to decreased renal excretion. Mild hypochloremia that is disproportionate to sodium suggests selective chloride loss as with vomiting (HCl loss), though this was not provided in the history. Bicarbonate is very low indicating a metabolic acidosis. The very high anion gap indicates that this is a titration or acid gain type of metabolic acidosis likely due to renal acid retention and possibly lactic acidosis. Ethylene glycol (exogenous acid) should also be considered given the finding of calcium oxalate monohydrate crystals in the urine.
Marked hyperphosphatemia is probably due to decreased renal excretion. Some antifreeze products also contain a phosphate rust inhibitor which can contribute to the hyperphosphatemia. There is a marked azotemia (increased urea and creatinine in this case) that is classified as renal because the USG is <1.035 in the face of azotemia.
Mild hyperglycemia is likely due to stress or excitement. A slight hypercholesterolemia is unlikely to be significant.
Urinalysis
The USG is slightly above isosthenuria but the urine is not concentrated (>1.035 for cats), therefore ruling out a prerenal azotemia, but consistent with renal azotemia. Trace proteinuria and glucosuria may be due to renal tubular injury (tubules unable to absorb protein and glucose), however a previously higher magnitude of stress hyperglycemia exceeding the renal threshold (~15.5 mmol/L in a cat) cannot be ruled out as a cause of the glucosuria. The number of WBCs and epithelial cells is not unusual, particularly for a catheterized sample. Calcium oxalate monohydrate crystals (picket fence type) are highly significant and support the diagnosis of ethylene glycol (antifreeze) ingestion. Scant fat is a common finding in the urine of cats since their renal tubular epithelial cells contain more lipid than other species.
- Bill was in acute renal failure from ingestion of the nephrotoxin ethylene glycol. He was strictly an indoor cat but he had licked water containing antifreeze from a leaky hot water radiator in the house. The prognosis was extremely poor and Bill was euthanized.
Case 2. Hobbes
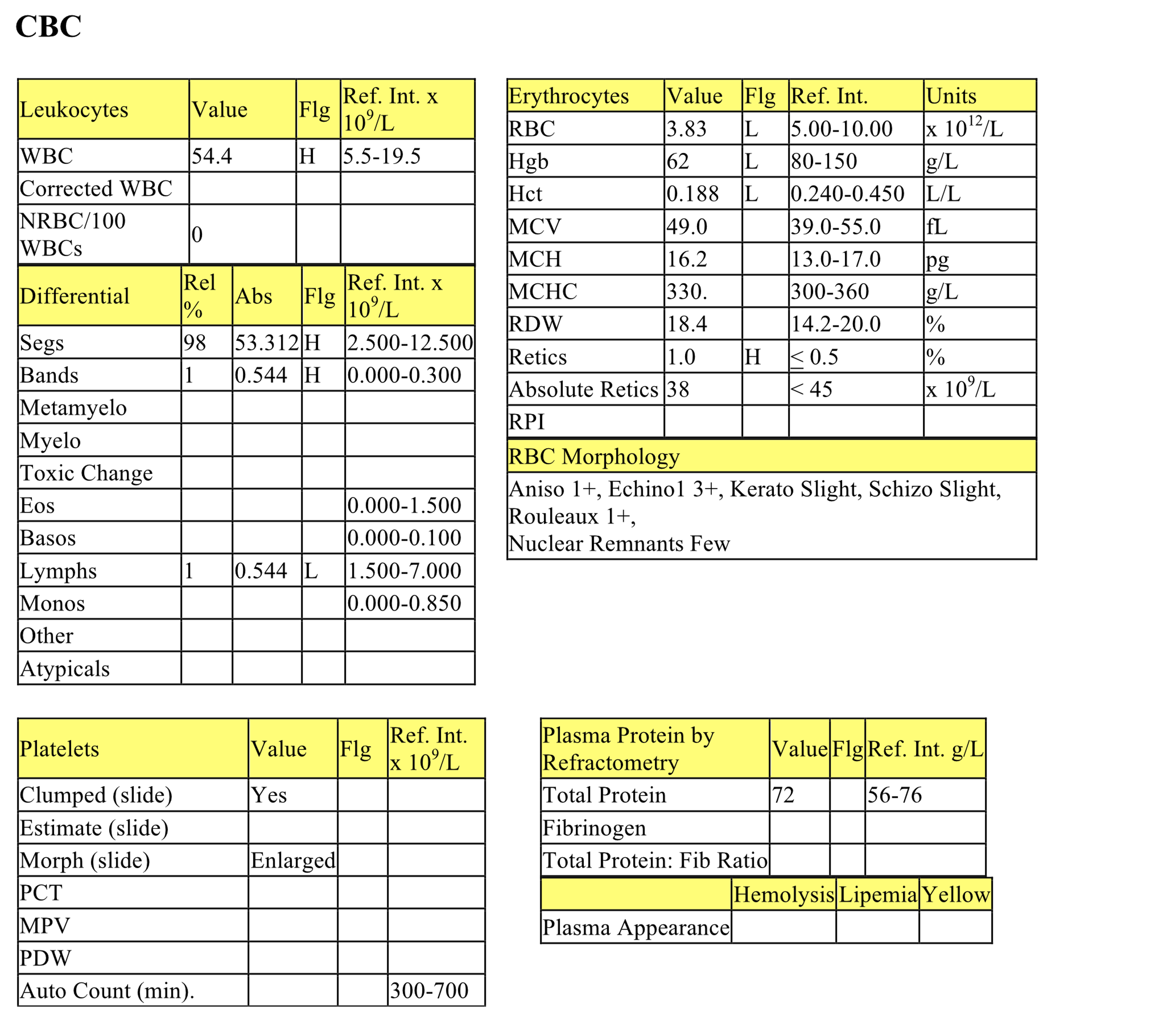
Hobbes, a 12-year-old M(c) DSH cat, had a history of polydipsia and weight loss for 2 weeks. Both kidneys were enlarged (egg-sized) on abdominal palpation.
CBC
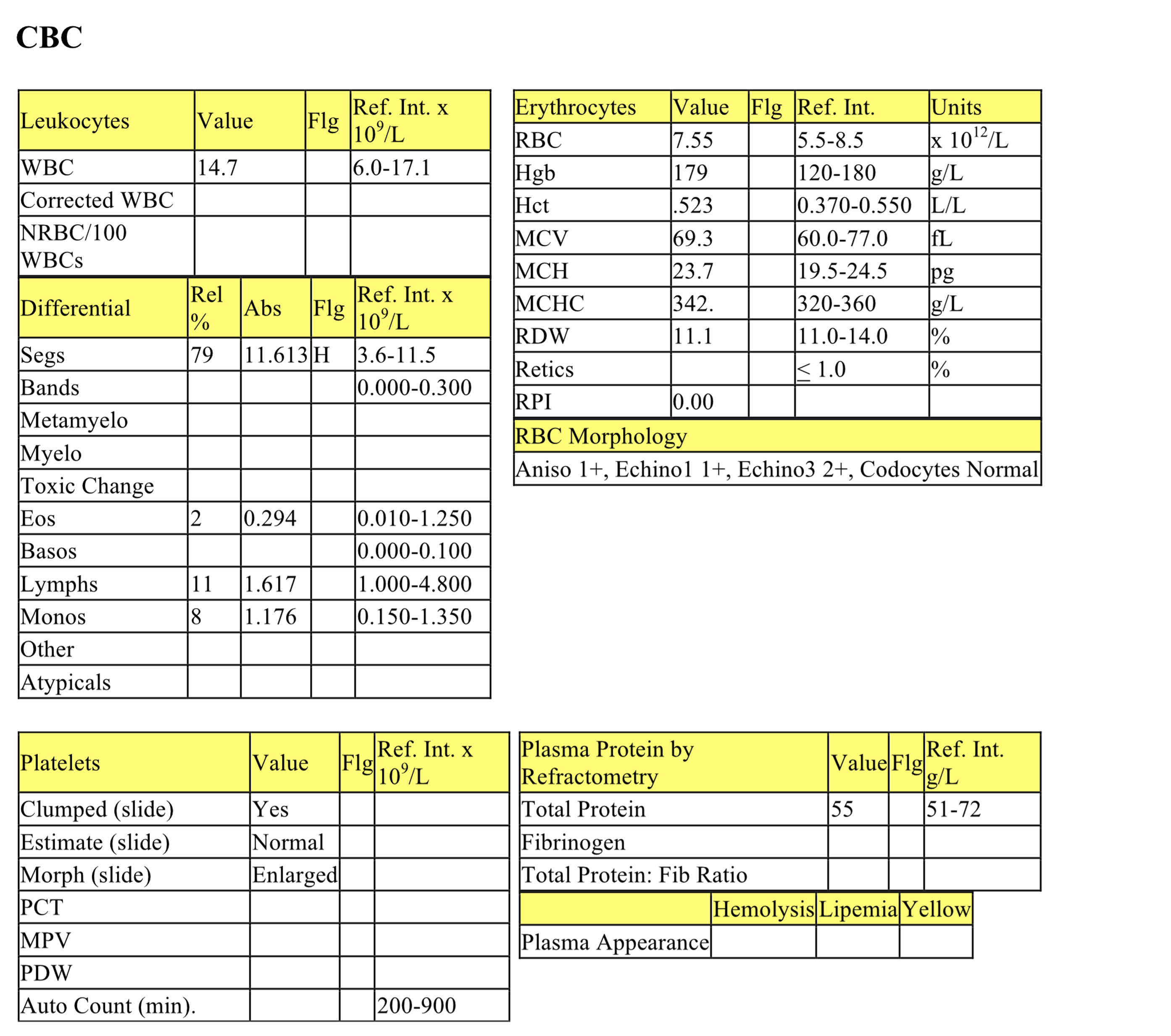
There is a mild to moderate nonregenerative anemia, and slight red cell pathology (keratocytes and schizocytes) suggestive of mechanical shearing of erythrocytes. The anemia could be due to chronic renal failure as well as inflammatory disease and underlying neoplasia, in this case (see below). The moderate to marked leukocytosis is characterized by a moderate/marked neutrophilia with a very mild left shift, suggestive of chronic inflammation. Moderate lymphopenia is due to stress of illness.
Biochemical Panel
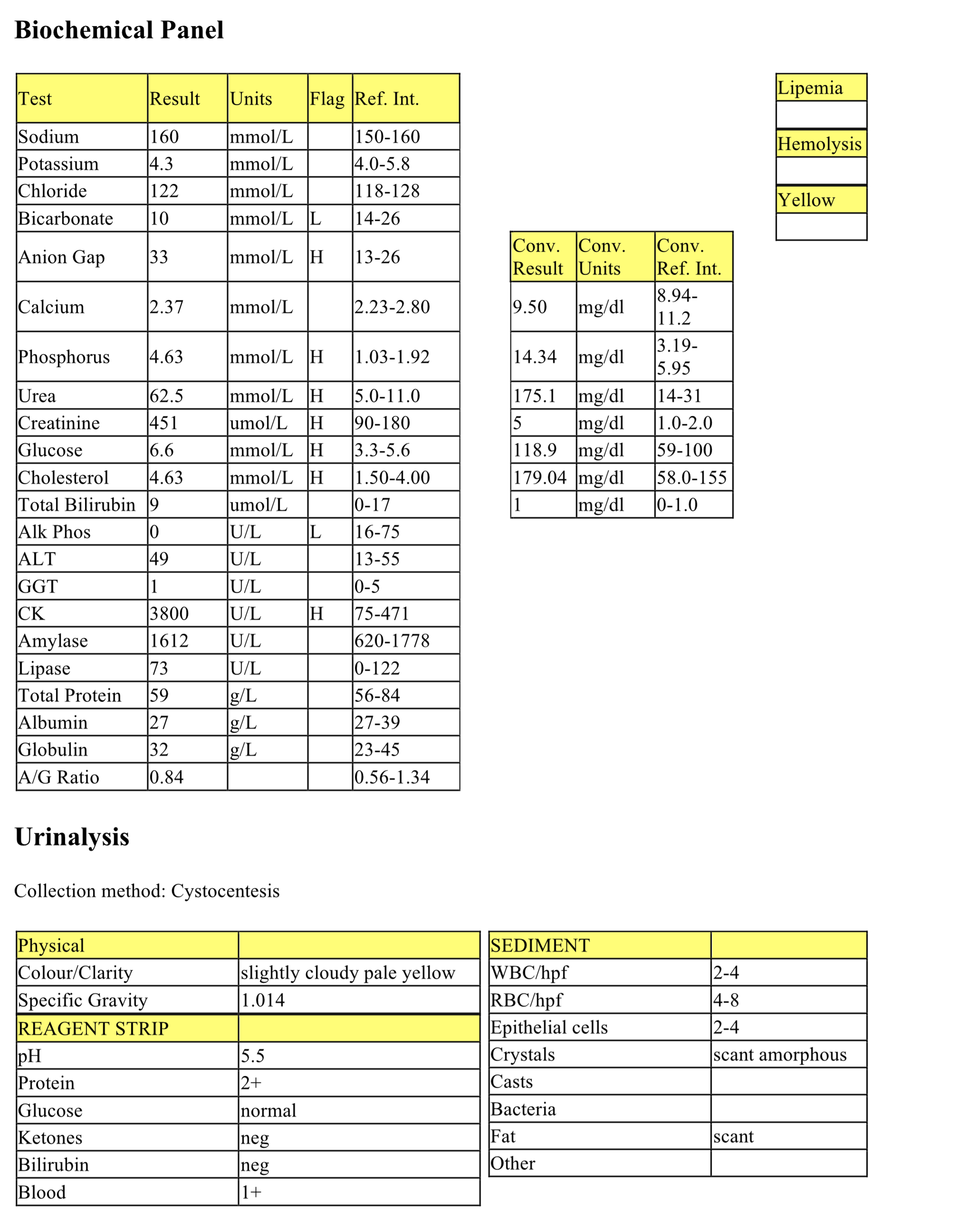
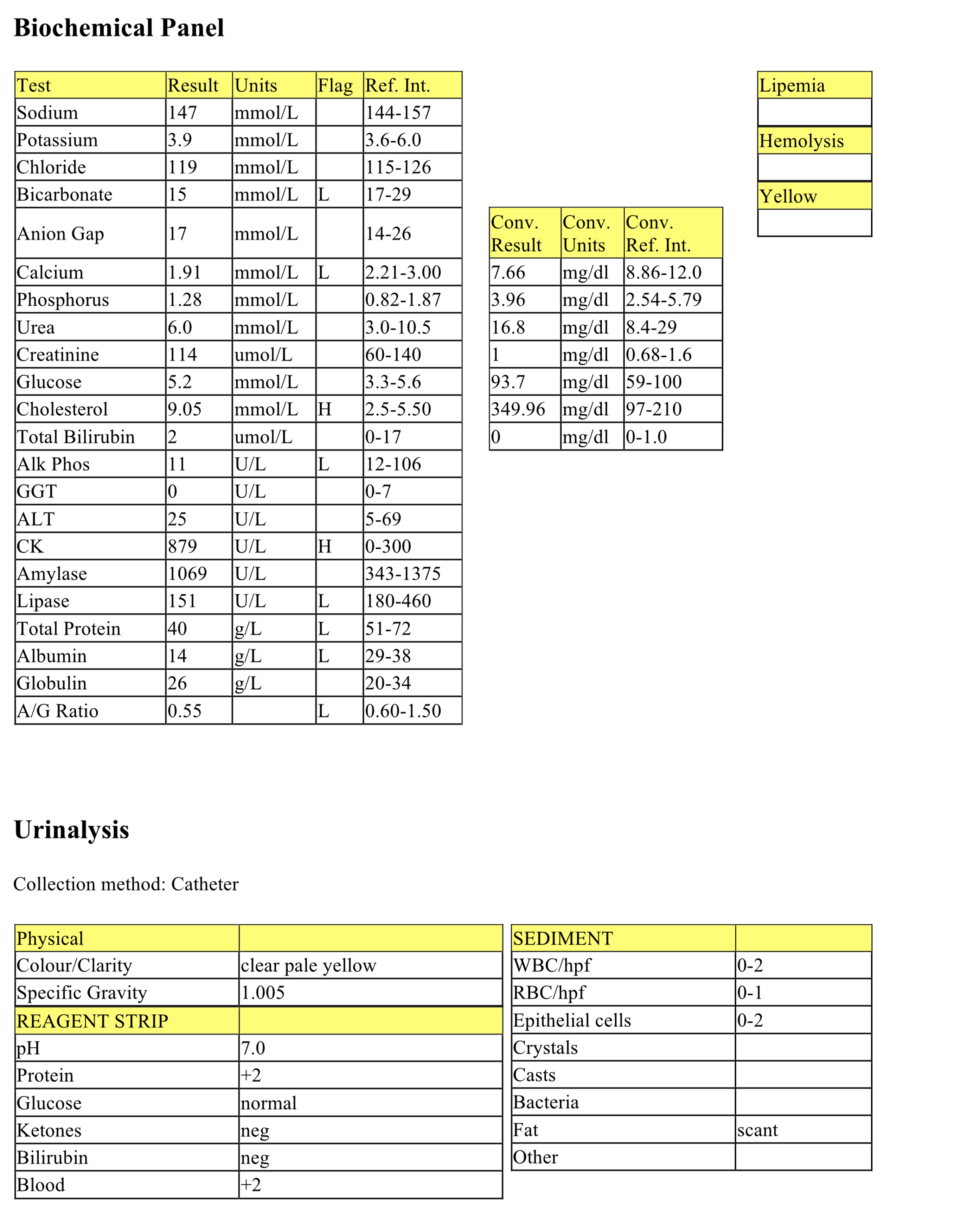
A mild decrease of bicarbonate along with an increased anion gap indicates a titration or acid-gain type of metabolic acidosis due, at least in part, to renal acid retention however lactic acid and exogenous acids, such as ethylene glycol, cannot be ruled out. Moderate hyperphosphatemia is due to decreased renal excretion. The moderate to marked azotemia is of renal origin since the urine is not concentrated. Mild hyperglycemia is likely due to stress or excitement. Mild hypercholesterolemia may be seen in a postprandial sample, and is otherwise a nonspecific abnormality. Low ALP activity is not clinically significant. Moderately increased CK activity indicates myocyte leakage/injury and this value is higher than typically explained by handling/venipuncture; therefore muscle trauma, hypoxia, IM injections must be considered as possible causes. Albumin is low normal, which may reflect loss in the urine given the finding of protein 2+ on reagent strip analysis of the urine.
Urinalysis
USG is slightly above isosthenuria but is not concentrated and in the face of azotemia indicates renal disease. The sediment is relatively inactive, therefore, the level of protein in the urine may be significant; measurement of a UPC is recommended to determine significance. The low number of RBCs and 1+ blood reading on the reagent pad may be secondary to the method of collection (cystocentesis) and would not be expected to interfere with the protein reading at this level.
- Although Hobbes was in renal failure, the kidneys were enlarged and there was an unexplained inflammatory leukogram. The degree of anemia may also be somewhat lower than usually seen with chronic renal failure alone in cats. The clinician re-examined Hobbes’ abdomen and could palpate a mass, possibly involving the intestinal tract. Both kidneys and the abdominal mass were aspirated and all three aspirates contained moderate numbers of large lymphocytes with prominent nucleoli, typical of lymphosarcoma. In addition, the abdominal mass aspirate contained a mixed population of bacteria. Hobbes was euthanized and the practitioner performed a necropsy. The mass involved the intestinal wall and there appeared to be a walled off abscess where leakage from the gut had occurred. The kidneys were white and irregular. The kidneys were fixed in formalin and submitted for histology which confirmed the diagnosis of lymphosarcoma.
Case 3. Marina
Marina, a 4-year-old Maine Anjou X cow, had a history of distancing herself from the herd and walking with a stiff gait for 2 days. Physical examination revealed a static gut, sawhorse stance, and a mucoid, red-tinged discharge from the vulva.
CBC
The hematocrit is low normal, which could represent a mild anemia for this cow (discussed below). The WBC count is low normal with mature neutrophils well within the RI, and a mild left shift with slight toxic change suggesting inflammation. Moderate lymphopenia is due to the stress of illness. Marked hyperfibrinogenemia and total protein to fibrinogen ratio <10 also indicate inflammation. Total protein in plasma is higher than total protein in serum due to the presence of fibrinogen, which is removed along with the blood clot when harvesting serum. The yellow appearance of plasma is due to dietary pigments, such as beta-carotenes and does not reflect icterus (see serum bilirubin result).
Biochemical Panel
The mild hypochloremic metabolic alkalosis is probably from HCl pooling in the abomasum. Abomasal stasis is a common finding in ill ruminants that may be inappetent or anorexic. Primary abomasal disorders also result in this acid-base disturbance, but usually the hypochloremia and alkalosis are more dramatic. Moderate azotemia is classified as renal because the USG is not concentrated (>1.025) and, in fact, is in the isosthenuric range. Moderate hyperglycemia is consistent with the stress of illness. Elevated activities of GGT (mild) and SDH (moderate) are due to mild cholestasis/biliary hyperplasia and hepatocellular injury, respectively. Mild muscle injury accounts for increased activities of CK and AST, although AST can also be released from damaged hepatocytes. The mild hyperproteinemia, mild hypoalbuminemia, and moderate hyperglobulinemia could be due to inflammation causing increased acute phase proteins and gammaglobulin synthesis, and decreased albumin as a negative acute phase protein. The globulin value can be calculated by subtracting albumin concentration from total protein concentration (90 g/L – 29 g/L = 61 g/L, which is above the RI for globulins in cattle (32-52 g/L).
Urinalysis
Isosthenuria and azotemia indicate renal disease. The reagent pad indicates blood at >+3 and there were high numbers of RBCs seen on sediment examination; these findings, together with the red/cloudy appearance of the urine, indicate hematuria (intact RBCs in the urine). This level of hematuria as well as sediment findings of inflammation and infection may all be contributing to the protein +3 detected on the reagent pad. Trace glucosuria relates to hyperglycemia which is probably due to stress. Leukocytes and bacteria were detected on sediment examination indicating inflammation/infection within the urogenital tract. Although the sample was free flow collection, the constellation of findings and the number of WBCs and bacteria suggest that their presence is not due to contamination of the sample. Also, a cytospin preparation revealed abundant extracellular and intracellular cocci and coccobacilli. Many neutrophils were degenerate. The presence of granular casts indicates renal tubular injury.
- Marina was diagnosed with pyelonephritis and renal failure. She was treated for several days with fluids and antibiotics. She became increasingly recumbent and remained anorexic. Laboratory tests were repeated. Nonregenerative anemia was confirmed and interpreted as both anemia of inflammatory disease and renal failure. Creatinine continued to increase and urea remained the same. Creatinine is a better indicator of renal function in cattle because urea is utilized as a protein source through excretion in the intestinal tract. Hyperglycemia also increased dramatically, which can be an agonal change in seriously ill cattle. High numbers of leukocytes, some in clumps, were seen on repeat urinalysis. Many bacteria and granular casts were also seen on sediment examination. Marina was euthanized and submitted for necropsy. Both kidneys were tripled in size, ureters were markedly distended, and the bladder wall was thickened and red. Viscous, red-brown fluid was contained within the renal calyces, ureters, and bladder. The etiologic agent was Corynebacterium renale. Probably both acute and chronic inflammation were present.
Case 4. Phillip
Phillip, a 2-year-old M(c) Collie X dog, had a history of inappetence for 3 days and swelling of the limbs. Physical findings included edema of the legs and ventral chest, and ascites.

CBC
The CBC is generally unremarkable. Echinocytes may be artifactual in this case. Mild neutrophilia is equivocal and, given the lack of a left shift and/or toxic change, its significance is questionable.
Biochemical Panel
The mildly decreased bicarbonate and normal anion gap indicate a mild secretory type metabolic acidosis that is likely due to renal bicarbonate loss. Mild hypocalcemia relates to hypoproteinemia, particularly hypoalbuminemia, since about 40% of calcium within the serum is protein bound. Although there are many potential causes of hypercholesterolemia, protein-losing nephropathy is a likely cause in this case (see below). Decreased lipase and ALP activities are not clinically significant. Mild increase of CK activity indicates myocyte injury that may be due to handling/restraint for venipuncture, although other causes of muscle injury cannot be ruled out.
Moderate hypoproteinemia due to hypoalbuminemia, along with +2 protein in the urine, suggests glomerular leakage of albumin (and possibly other low molecular weight proteins) into the urine. This dog’s clinical history of edema and ascites is likely due in part to the hypoalbuminemia and resulting decrease in oncotic pressure.
Urinalysis
The USG is hyposthenuric, which is not necessarily concerning since there is no azotemia present. Protein at +2 is likely to be significant at this low specific gravity; however, UPC is recommended. The sediment is inactive and does not explain the proteinuria. The presence of +2 blood may reflect collection of urine via catheterization.
UPC
The UPC of almost 14 is very high and supports a diagnosis of protein-losing nephropathy. Glomerulonephritis and renal amyloidosis are the two main differentials for proteinuria of this magnitude.
- Phillip was diagnosed with protein-losing nephropathy and was treated with corticosteroids and supportive care for several weeks, but ultimately deteriorated and was euthanized. The final diagnosis was: membranous glomerulonephritis, diffuse, moderate, and chronic. This case demonstrates the fact that severe glomerular pathology leading to protein-losing nephropathy and serious illness can occur without concurrent azotemia and isosthenuria. The combination of proteinuria, hypoalbuminemia, third space loss of fluid (ascites in this case), and hypercholesterolemia is referred to as nephrotic syndrome and is pathognomonic for glomerular disease.
Case 5. Tyrion
Tyrion, a 4-year-old M Pekingese X dog, had a history of vomiting, lethargy, and weakness for 1 day. On physical examination, he had a very tense abdomen, feces around the anus, and blood dripping from the penis. Urine could not be obtained.
CBC
The mild increase of hematocrit, hemoglobin, and high normal RBC count suggest relative erythrocytosis due to dehydration +/- splenic contraction. The WBC count and neutrophil numbers are within RI, however, there is a mild left shift with toxic change suggesting acute inflammation. Moderate lymphopenia indicates stress.
Biochemical Panel
Low sodium and chloride are due to movement of these electrolytes from the vasculature into the abdominal cavity. Hyperkalemia is a result of movement from the high potassium fluid in the abdomen (i.e. urine) into the intravascular space. High anion gap metabolic acidosis is from renal acid retention and possibly a gain of lactic acid. Mild hypocalcemia may result from hyperphosphatemia. Moderate hyperphosphatemia is due to decreased renal excretion. Increases in urea and creatinine indicate azotemia, postrenal in this case. Hypoglycemia is not from in vitro glycolysis as the serum was separated quickly. Sepsis is a likely explanation for the hypoglycemia. The cause of the mild hypercholesterolemia is not known. The increased ALP activity could be from cholestasis or steroid induction. Increased CK activity indicates mild muscle injury. Decreased lipase activity is not clinically significant.
Abdominal Fluid
This hemorrhagic fluid has a nucleated cell count which is higher than peripheral blood and is likely to represent an exudate (protein not determined). Degenerate neutrophils were present, as were both intracellular and extracellular cocci.
Urea and Creatinine of abdominal fluid
The urea and creatinine of the abdominal fluid are both higher than their serum values; however, creatinine is disproportionately higher relative to urea.
- Tyrion had a ruptured urinary tract. Septic peritonitis does not occur with urine leakage unless sepsis pre-exists in the urogenital tract when the rupture occurs. Traumatic rupture, with no predisposing cause, results in a fluid with a very low protein content and nucleated cell count (transudate). Tyrion was euthanized and at necropsy was found to have: urolithiasis with severe hemorrhagic cystitis and ruptured bladder; uroabdomen; prostatitis with intralesional Gram positive cocci; tubulointerstitial nephritis, suppurative with intralesional Gram positive cocci; and aspiration pneumonia, acute and severe.
Number of erythrocytes per liter of whole blood (measured).
Increased number of erythrocytes with decreased volume that usually corresponds with decreased MCV; often associated with iron deficiency as well as portosystemic shunts.
Average erythrocyte size in femtoliters (measured or calculated PCV or Hct÷RBC).
Variation in cell size.
Increase in the number of neutrophils in peripheral blood.
Increase in the number of monocytes in peripheral blood.
Typical change seen in peripheral blood of an ill or stressed animal (with increased cortisol levels), consisting of lymphopenia which may be accompanied by neutrophilia and monocytosis (species differences exist).
Method of measuring the protein content of a fluid that relies on refraction of light, which is proportional to the quantity of solids in solution.
Crescent-shaped cells that are formed from mechanical shearing (usually due to fibrin strand deposition) of the red cell.
An erythrocyte fragment created by shearing trauma to erythrocytes within the vascular system; often the fragment which has been sheared off to form a keratocyte.
Release of less mature neutrophil stages (bands, metamyelocytes, myelocytes) from the marrow into the peripheral blood in response to inflammation.
Mononuclear, non-phagocytic leukocyte responsible for humoral (B lymphocyte) and cell-mediated (T lymphocyte) immune responses.
Cytoplasmic abnormalities seen in neutrophils that have not matured normally in the bone marrow. Abnormalities include retention of primary granules, vacuolation, darker staining due to retention of ribosomes, and deposits of rough endoplasmic reticulum (Döhle bodies).
Jaundice; deposition of pigment in skin, mucous membranes and sclera due to hyperbilirubinemia; usually results in a yellow discoloration of skin and mucous membranes.
Impaired bile flow.
Cellular proliferation- increased number of normal cells.
Nonspecific term for sublethal or lethal injury to hepatocytes due to various causes, e.g. hypoxia, toxins, infection.
Method of preparing a concentrated sample for evaluation of cell poor fluids.
Erythrocyte with even projections all around its membrane; often an artifact but can be a pathologic change. Echinocytes are classified as types 1 and 3 depending on the length and sharpness of the projections (spicules).
Increase in hematocrit (PCV) in peripheral blood; usually accompanied by increases in hemoglobin and RBC numbers.
Granulocyte with fine, inconspicuous cytoplasmic granules and a segmented nucleus; important in phagocytosis and killing of bacteria.
Fluid with an elevated protein concentration and nucleated cell count.
Term used to describe neutrophils in cytologic preparations indicating swelling and lysis of the neutrophil nucleus, e.g. due to bacterial infection.
Very low protein, cell poor fluid.
