
Case Studies
Case 1. Trish
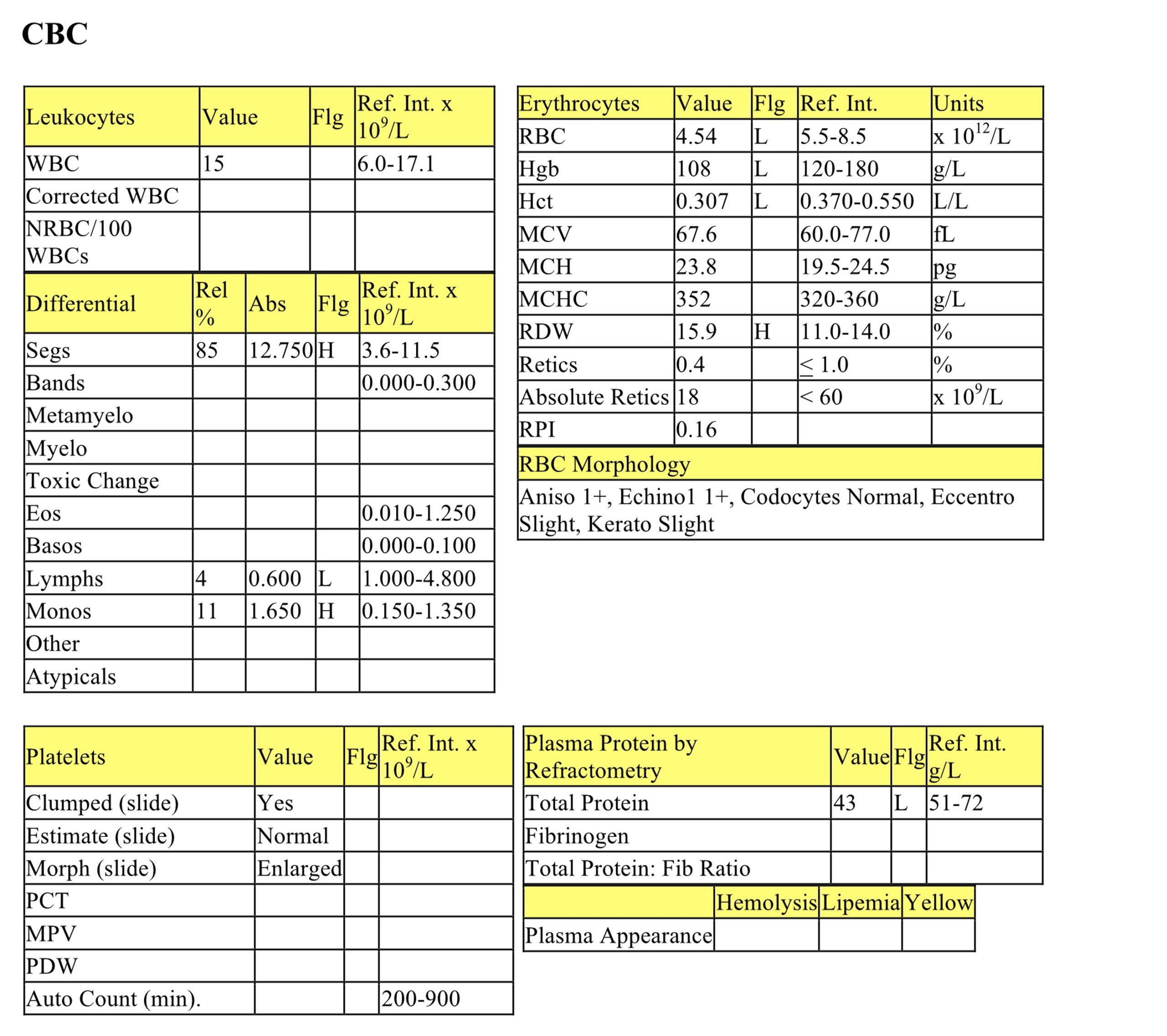
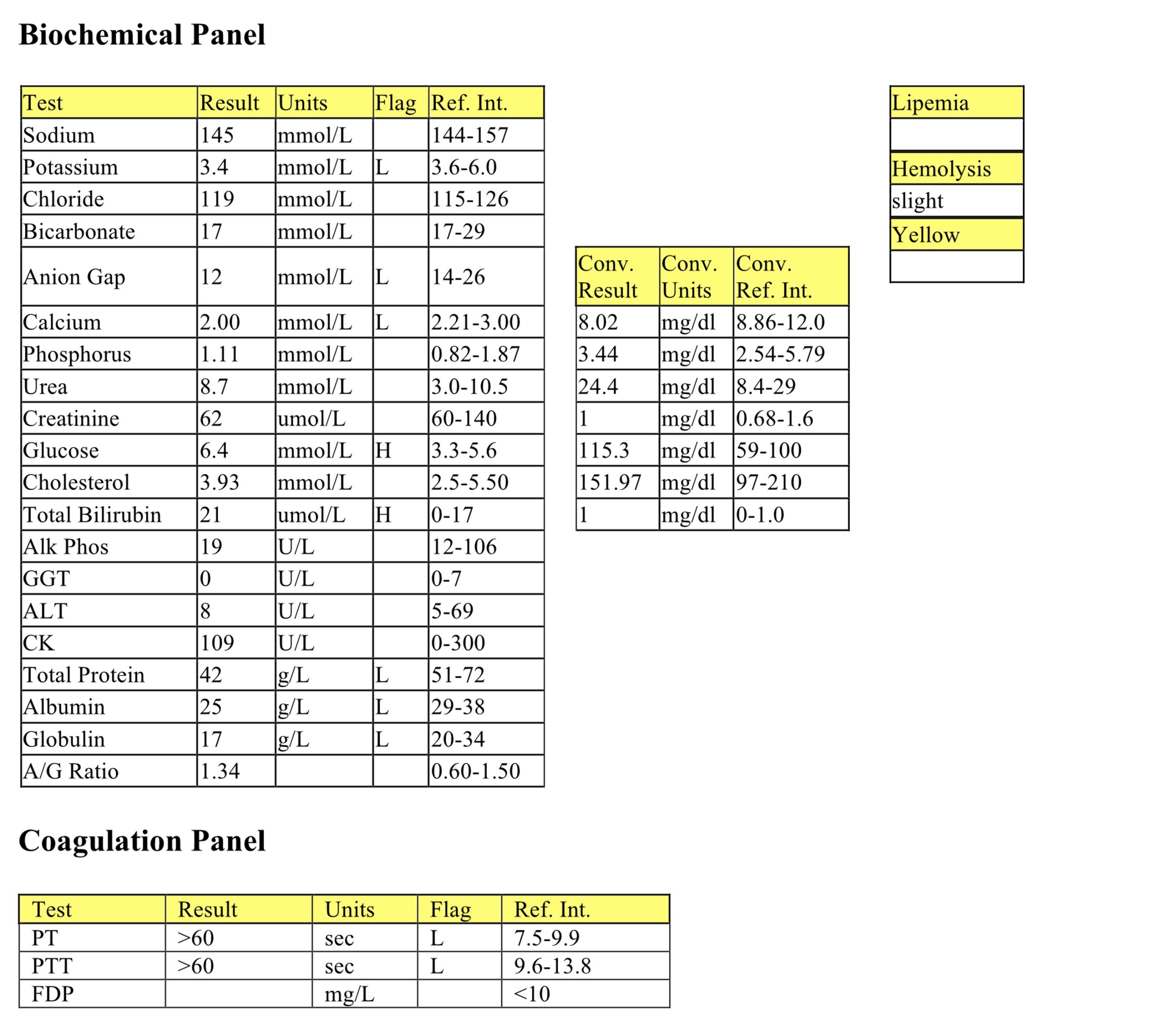
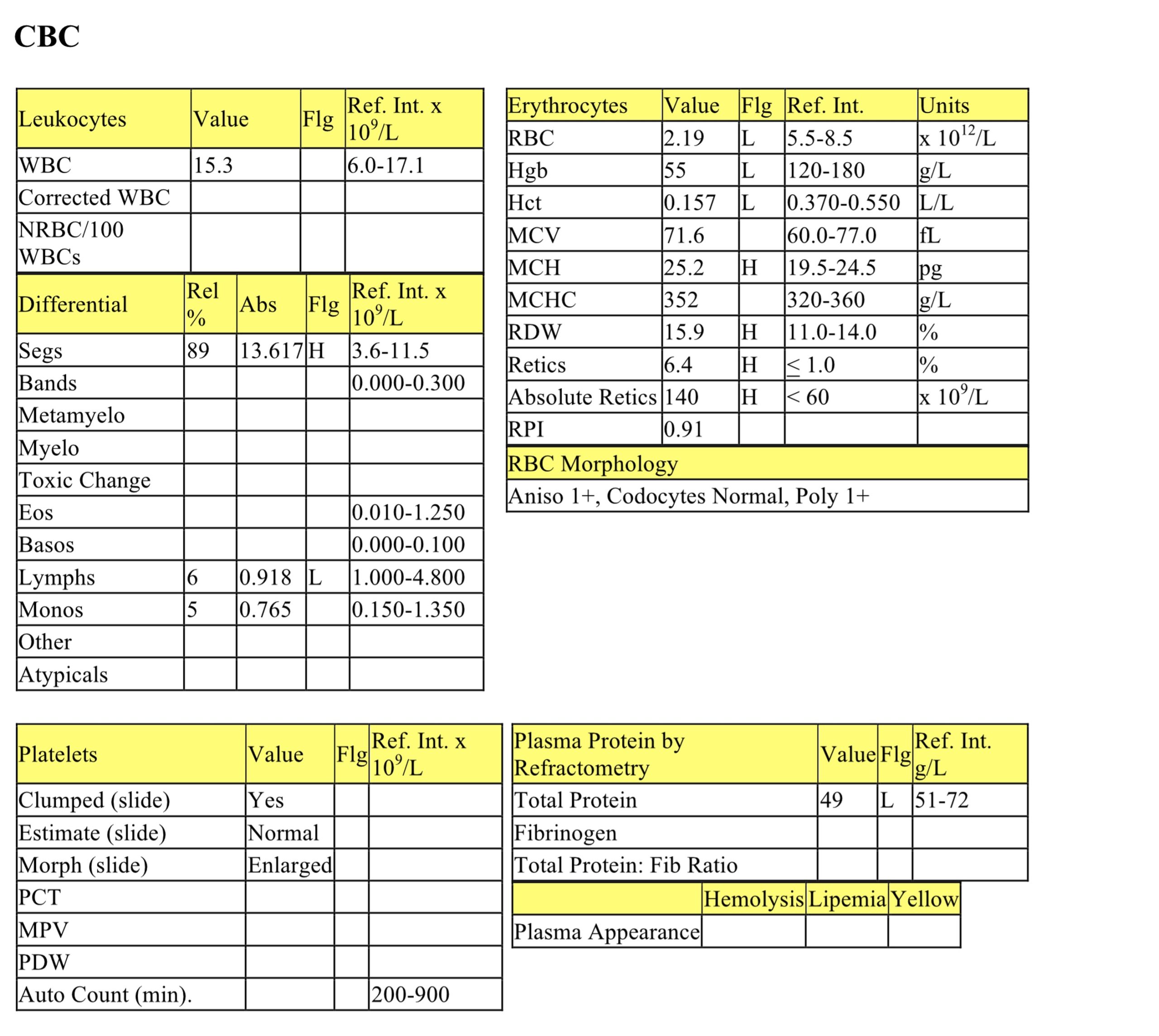
Trish, a 1-year-old F Miniature Poodle x dog had a 3 day history of lethargy, wheezing, coughing, and decreased food and water intake. Six mL of bloody fluid was removed from the chest cavity.
CBC
Trish has a mild to moderate nonregenerative anemia. Slight red cell pathology is present (eccentrocytes and keratocytes), but the significance in this case is questionable. The mild neutrophilia, moderate lymphopenia and mild monocytosis are consistent with a classic stress response. See biochemical panel interpretation for protein interpretation.
Biochemical Panel
Mild hypokalemia is probably a result of lack of intake. Low anion gap and calcium are due to low albumin. Free calcium (the active form) is not affected by hypoalbuminemia. Mild hyperglycemia is likely due to stress. Mild hyperbilirubinemia could result from internal hemorrhage and increased delivery of RBC breakdown products (e.g. bilirubin) to the liver. Hypoproteinemia noted on the CBC is due to panhypoproteinemia. Anemia and hypoproteinemia could be due to acute/ongoing hemorrhage.
- Thoracocentesis revealed a hemorrhagic effusion.
- Coagulation tests indicate defects in the intrinsic and extrinsic pathways, the common pathway, or multiple defects. The history and clinical and laboratory findings are highly suggestive of vitamin K antagonism.
- Additional questioning confirmed that Trish had been off leash in an area where exposure to a warfarin-like rodenticide was possible. These products affect factors II, VII, IX, and X resulting in the synthesis of nonfunctional proteins that are unable to bind calcium. Newer rodenticides can affect these factors for several weeks requiring that vitamin K1 be administered for at least 4 weeks. Factor VII is affected first following ingestion of vitamin K antagonists, causing the PT to be prolonged before the PTT. However, by the time animals are clinically affected (bleeding), usually both PT and PTT are prolonged. As an acquired coagulopathy, the bleeding is consistent with a disorder of secondary rather than primary hemostasis. Large spreading hematomas and bleeding into body cavities and joints are seen rather than small hemorrhages from mucosal and other superficial surfaces.
- Trish was given fresh plasma to restore coagulation factors, vitamin K to counter the effect of the rodenticide, and supportive care. PT and PTT were repeated on day 3 and values were within RI. A CBC was not repeated but one would expect erythroid regeneration to start occurring.
Case 2. Marble
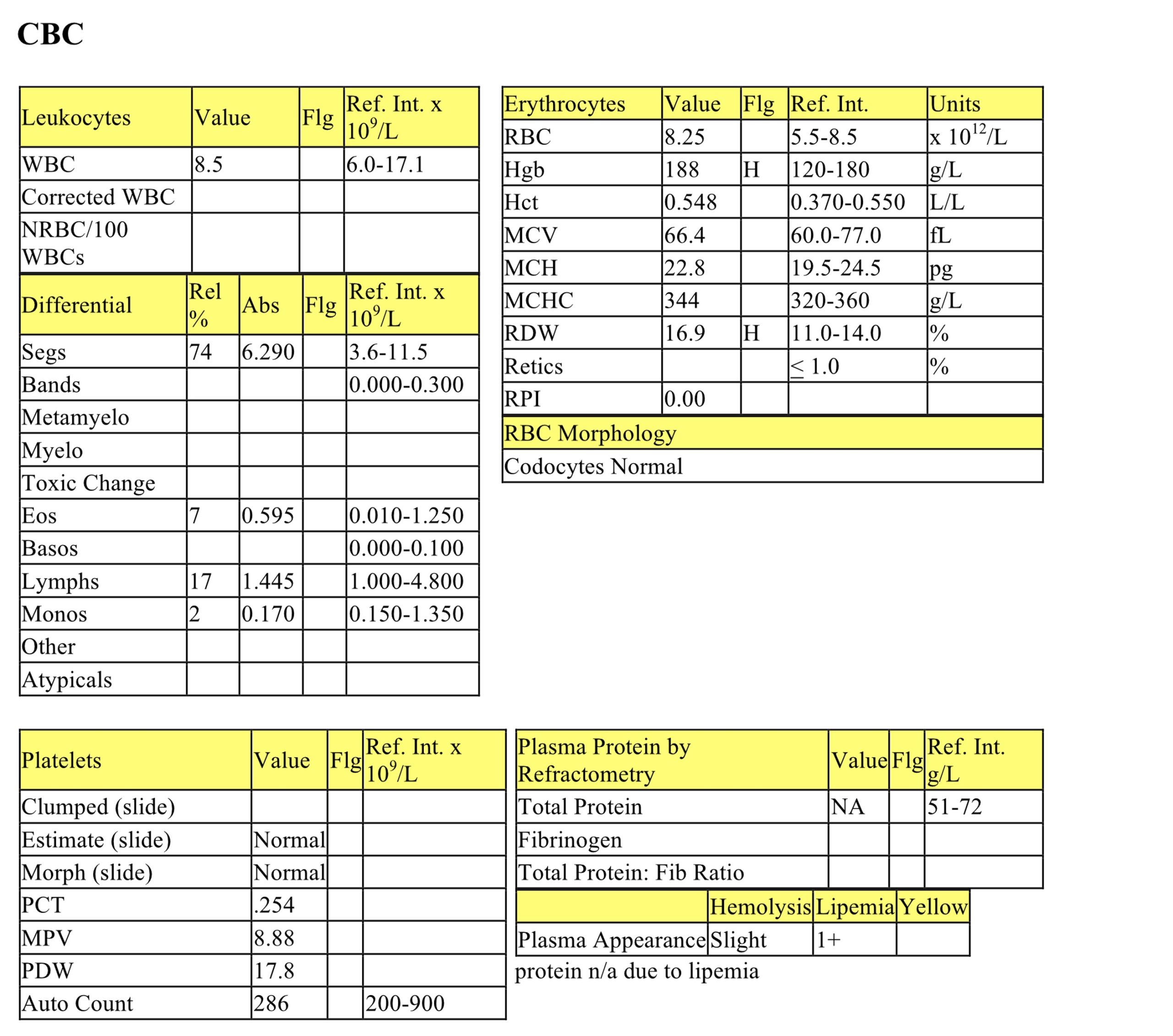
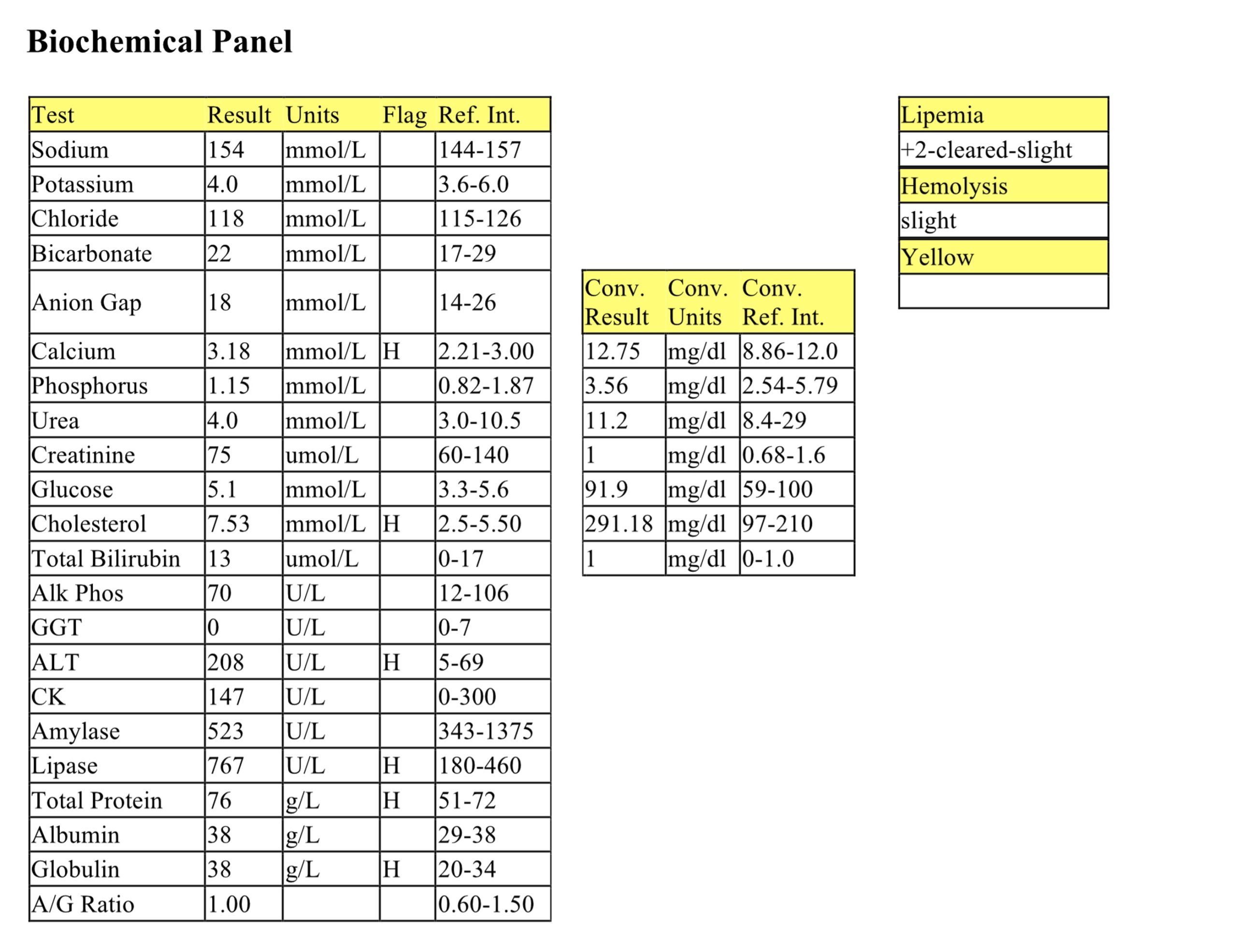
Marble, a 9-year-old Doberman Pinscher dog, had epistaxis for 1 day. She had been given one aspirin on the morning of presentation to the clinic.
CBC
The hematocrit is at the upper end of the RI which may be normal for this patient or due to mild dehydration. The remainder of the CBC is unremarkable. Lipemia is likely from postprandial sampling.
Biochemical Panel
Mild hypercalcemia may be related to mild hyperproteinemia and increased binding of calcium to protein. Free calcium, the functional form, is unaffected by this increased binding. The hypercholesterolemia is unlikely to be clinically significant and could relate to recent feeding. The mild increase in lipase activity may also be insignificant given the lack of inflammation on the leukogram, normal amylase activity, and the lack of history to suggest pancreatitis. Mildly increased ALT activity indicates mild hepatocellular injury. Hyperproteinemia, high normal albumin, and normal albumin to globulin ratio suggest mild volume contraction (dehydration).
Epistaxis can be associated with defective hemostasis (usually, but not exclusively, primary hemostasis), or a local lesion or inflammation. Platelet numbers are within the RI; therefore, thrombocytopenia is ruled out as a cause of superficial bleeding. A vascular defect, platelet function defect, or defect of primary hemostasis extrinsic to the platelet (e.g. vWD) should be considered. Although the type of bleeding is less suggestive of a coagulopathy (disorder of secondary hemostasis), activated clotting time (ACT) was done to evaluate the intrinsic and common coagulation pathway. The ACT was 50 seconds (RI <2 minutes). BMBT is indicated when a disorder of primary hemostasis is suspected and thrombocytopenia has been ruled out. The BMBT was 8 minutes (RI <4 minutes). vWF was 16% (RI 45 – 180%) and a diagnosis of vWD was made.
- If vWD had been ruled out, platelet function tests would have been performed. Marble had previously been spayed and had lipomas removed. Excessive bleeding and delayed healing had complicated the lipoma surgery. No information was available regarding the ovariohysterectomy procedure. Despite the diagnosis of vWD, thorough examination of the nasal cavity would be advisable. A lesion or inflammation resulting in increased vascular permeability could aggravate clinical bleeding in a dog with vWD.
Case 3. Larry
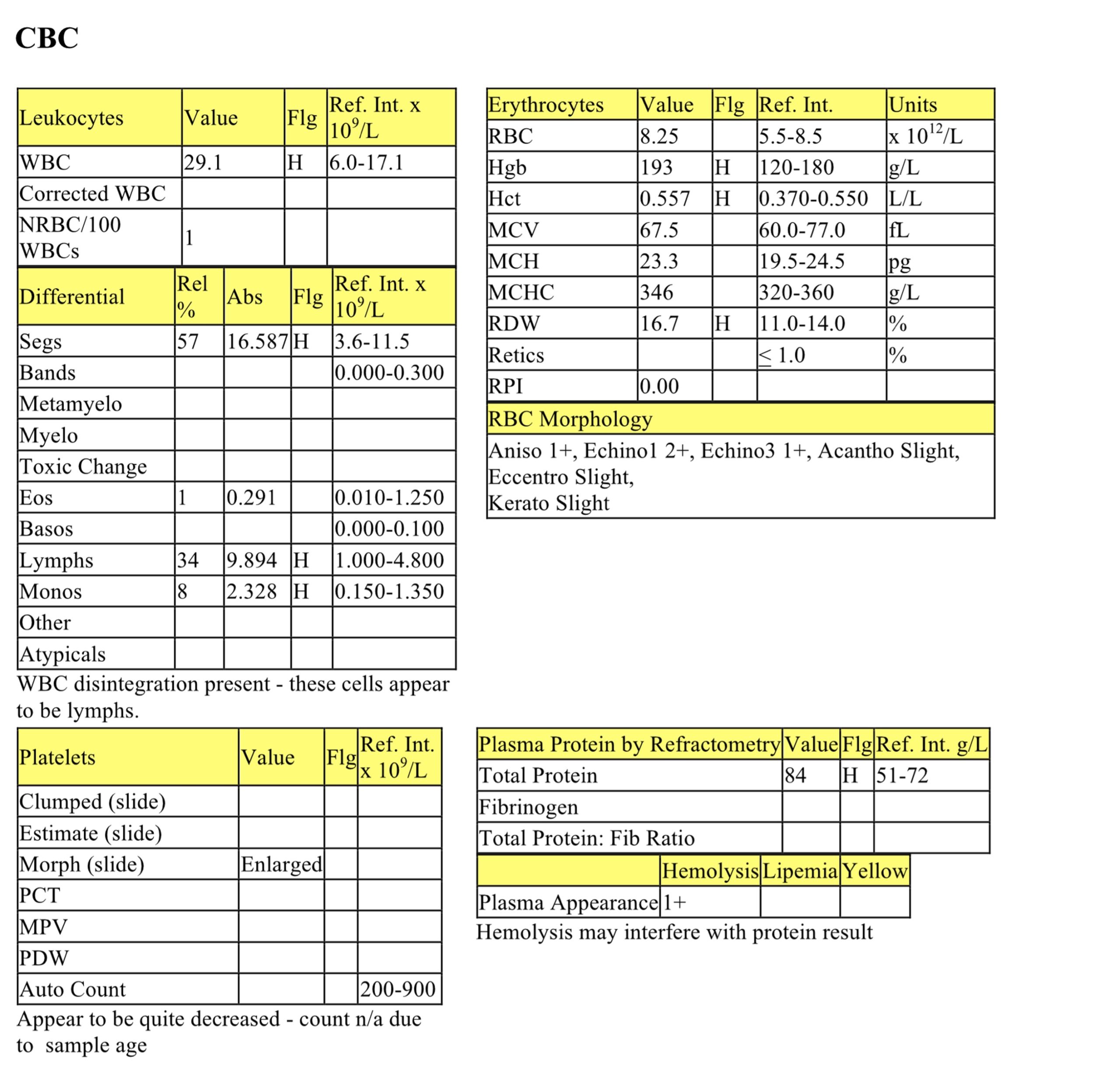
Larry, a 1-year-old M Pomeranian dog, had severe bruising in the right inguinal area. A similar problem had occurred 2 months earlier.
CBC
Larry has a severe anemia that is mildly regenerative, based on increased polychromasia, reticulocyte %, and reticulocyte absolute count; however, the RPI has not reached a level that indicates regeneration. The mild neutrophilia and mild lymphopenia could be explained by stress. See below for the protein interpretation.
Biochemical Panel
Moderate hyponatremia and hypochloremia could result from hemorrhage. Mild hypokalemia could be due to increased losses as well as decreased intake. Low anion gap relates to hypoalbuminemia (decreased “unmeasured” anion). Mild hypocalcemia is also due to hypoproteinemia. The mild urea elevation could be prerenal if perfusion of the kidneys is poor. Low or decreased muscle mass could explain the lack of concurrent creatinine elevation. Intestinal hemorrhage can also explain elevated urea together with a normal creatinine, however, there was no history of intestinal bleeding in this case. Mild hyperglycemia is likely from stress. Low amylase and lipase activities are not clinically significant. The mildly increased ALP activity may relate to bone turnover/growth in this young dog. Hypoproteinemia involves all protein fractions (normal albumin:globulin) which supports an etiology of recent/ongoing blood loss.
Coagulation Panel
Prolongation of PTT with normal PT focuses the problem on the intrinsic system. A congenital coagulopathy was suspected and sex-linked factor VIII deficiency would be most common. Larry’s factor VIII activity was 2.4% (RI 50-200%), confirming hemophilia A. The gene for factor VIII is on the X chromosome and factor VIII deficiency is recessive. The dam is a carrier of hemophilia A and about half of her male offspring are clinically affected. One half of her female offspring will carry the abnormal gene.
- Despite several fresh whole blood and plasma transfusions, Larry succumbed to massive intrathoracic and intrapulmonary hemorrhages about 3 months following the diagnosis.
Case 4. Charisse
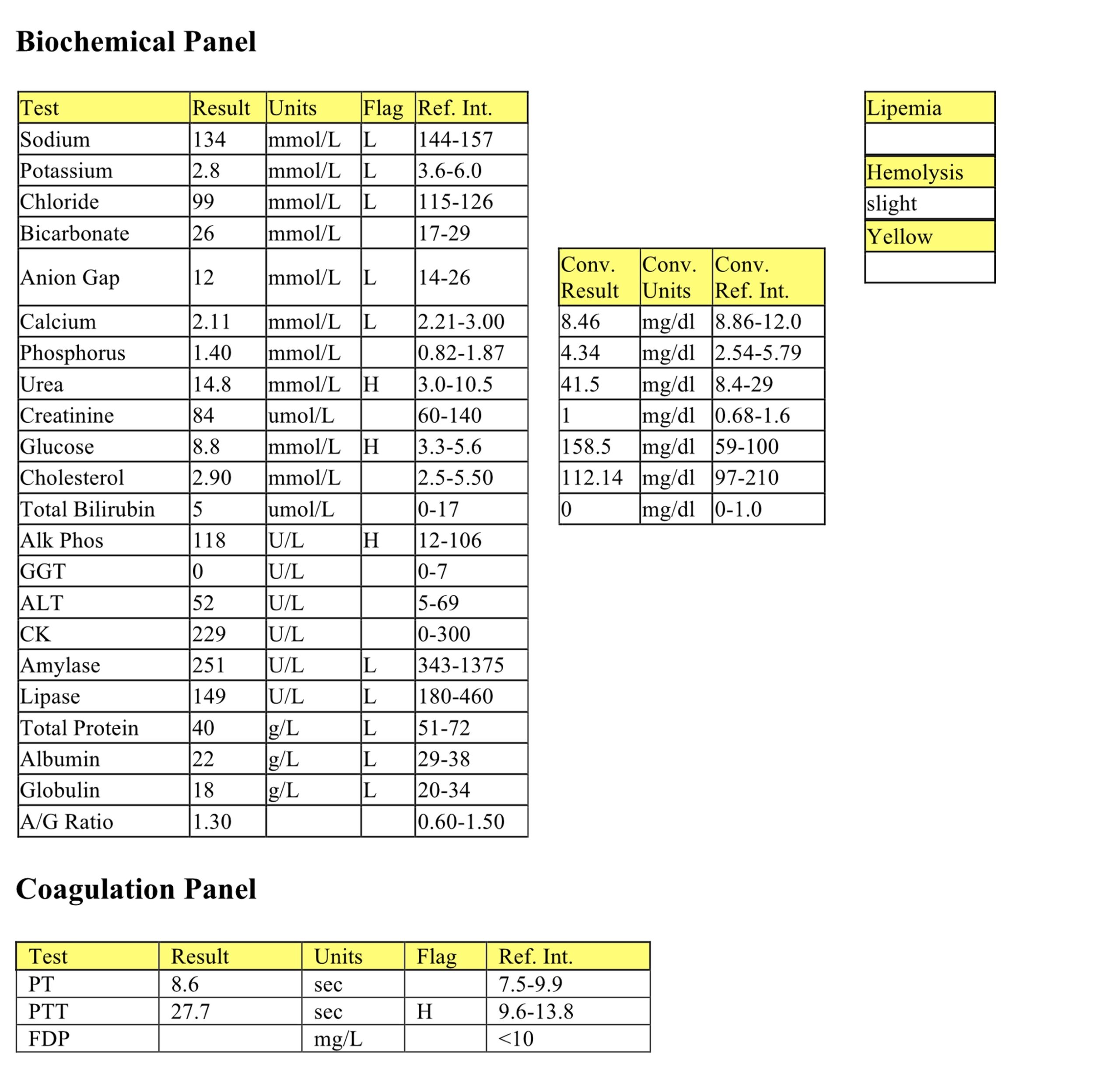
Charisse, a 6-year-old Appaloosa mare, had a history of nasal discharge, epistaxis, and edema of all four limbs. Physical findings included enlarged submandibular lymph nodes.
CBC
Charisse has a mild to moderate anemia which may be nonregenerative given the lack of MCV and RDW elevation, and the other laboratory findings. However, given the species one cannot be certain based on these findings alone. Despite a moderate leukocytosis, there is a severe neutropenia and the majority of leukocytes are atypical monocytoid cells. Severe thrombocytopenia is also present and this most likely explains the epistaxis noted in the history. Hyperproteinemia could be better characterized on a biochemical panel. However, dehydration, increased acute phase proteins, and increased gammaglobulins would all be possible. The fibrinogen is elevated and the protein to fibrinogen ratio indicates there is an absolute hyperfibrinogenemia. These findings suggest concurrent inflammation, which could be secondary to increased susceptibility to infection resulting from the severe neutropenia.
The CBC findings are consistent with leukemia, possibly monocytic, and cytopenias due to the presence of neoplastic cells in the bone marrow (myelophthisis).
Aspirated bone marrow was highly cellular. Monocytoid cells resembling those in the peripheral blood predominated and there was a lack of all normal hemopoietic tissue. Results of cytochemical staining facilitated the diagnosis of monocytic leukemia. Similar cells were found in several organs and multiple lymph nodes at necropsy.
Case 5. Cubby
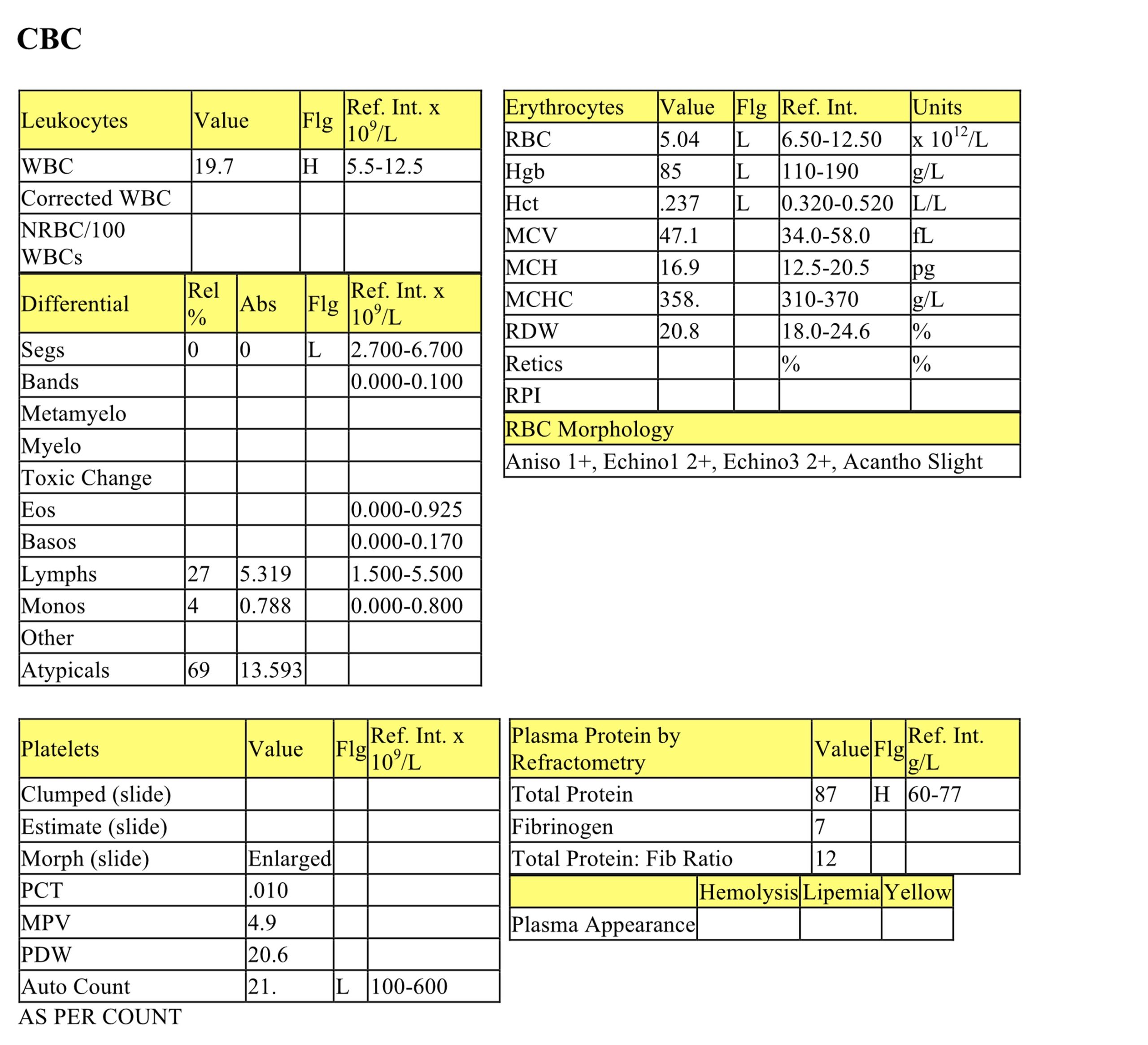
Cubby, a 3-year-old M(c) Golden Retriever dog, had anorexia, depression, and lethargy for 4 days.
Cubby, day 1

Day 1
CBC
The mildly increased hematocrit and total protein suggest mild dehydration. Mild RBC pathology is present, most notably echinocytes III which can be associated with azotemia (present here), electrolyte disturbances, or artifactual change. The moderate leukocytosis is due to mild neutrophilia, moderate lymphocytosis, and mild monocytosis. Lymphocyte disintegration suggests that a fragile cell population may be present. The lack of a stress lymphopenia in an ill dog could occur for several reasons, likely lymphoid neoplasia in this case. Thrombocytopenia could be due to several mechanisms such as: immune-mediated destruction, impaired megakaryopoiesis, sequestration, and consumption from DIC&F.
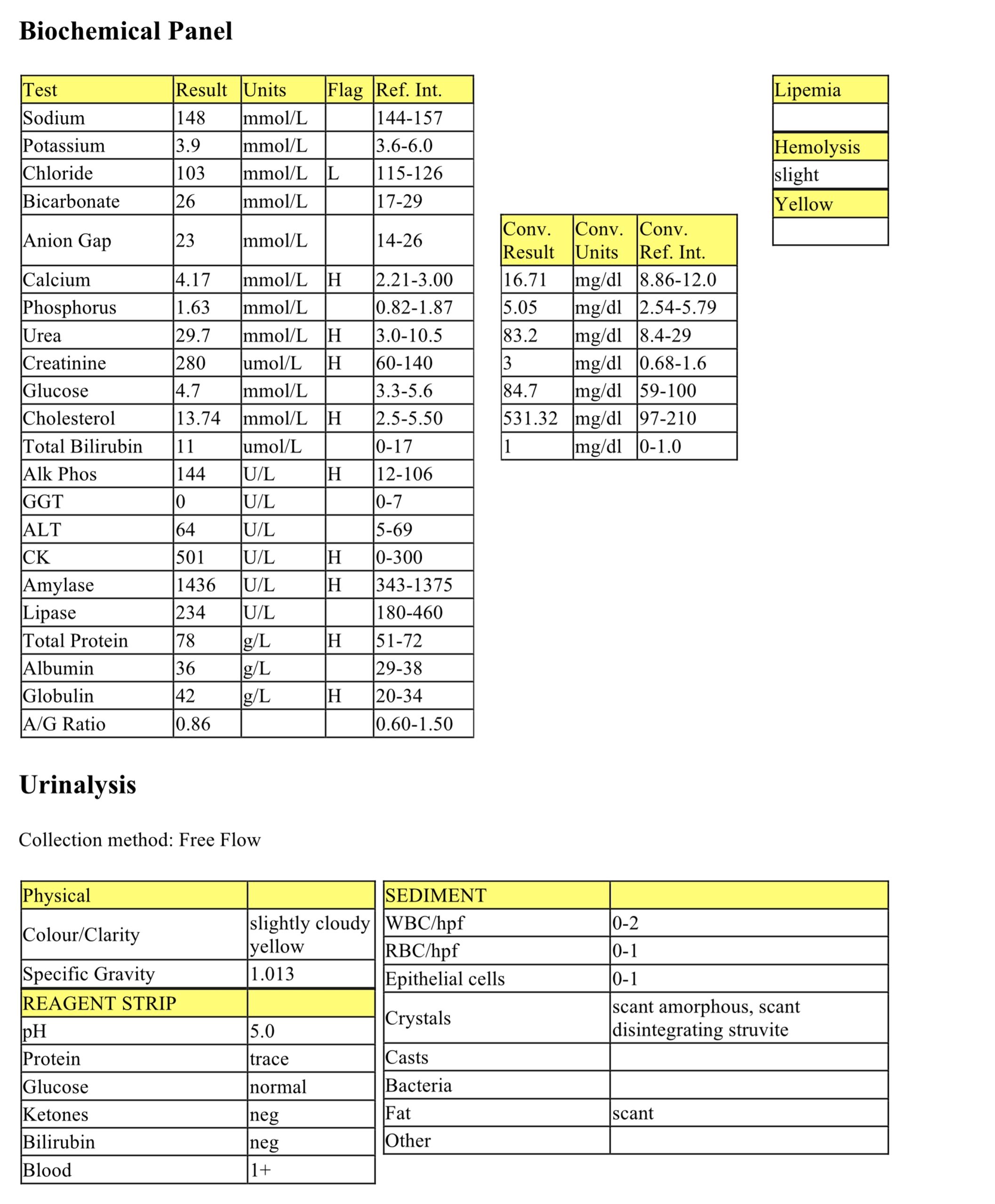
Biochemical Panel
Mild hypochloremia could be due to vomiting, although this was not in the history. Marked hypercalcemia is likely due to hypercalcemia of malignancy in this case. Azotemia in the presence of unconcentrated (approaching isosthenuric) urine indicates renal disease. Moderate hypercholesterolemia can occur with cholestasis, several endocrinopathies, disorders of lipid metabolism, protein-losing nephropathy, and hepatic disease; the mechanism in this case is not clear. Mild hyperamylasemia, in isolation, is unlikely to be clinically significant. The mild increase in ALP activity could be due to cholestasis, enzyme induction, or bone source. Mildly increased CK activity could be from handling and venipuncture. Mild hyperproteinemia could be from dehydration, although the albumin is within the RI. Contributions from increased acute phase proteins and/or immunoglobulins should also be considered.
Urinalysis
The urine is not concentrated and Cubby is azotemic, indicating renal disease. Hypercalcemia can lead to renal pathology and interference with antidiuretic hormone activity in the renal tubules. Alternatively, hypercalcemia can result from renal failure, particularly in young dogs with congenital renal disease. Given the evidence for lymphocytic leukemia on peripheral blood examination, hypercalcemia of malignancy causing impaired renal function is more likely than primary renal disease.
Cubby began vomiting blood and bleeding excessively from venipuncture sites during his first evening in hospital.
Coagulation Panel
Prolonged PT and PTT along with thrombocytopenia are highly suggestive of DIC&F. Cubby was transfused with fresh frozen plasma.
Day 2
CBC
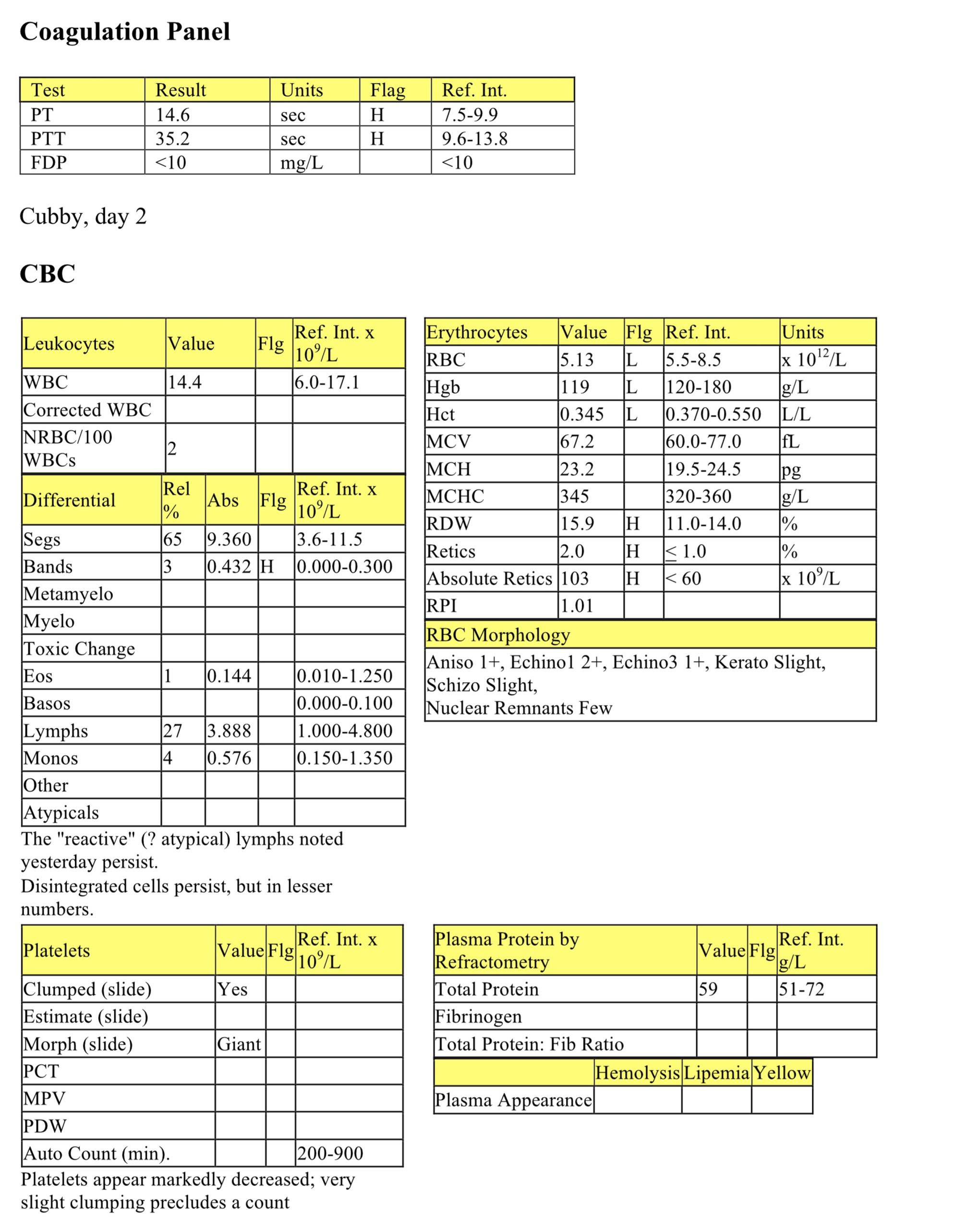
The drop in hematocrit and protein are consistent with hemorrhage and/or dilution from fluid administration. Slight keratocytes and schizocytes, thrombocytopenia, and the development of hemorrhaging support the diagnosis of DIC&F. There is now a mild left shift on the leukogram and, although lymphocytes have dropped, there is still no stress lymphopenia.
Coagulation Panel
PT and PTT are still prolonged; FDPs remain within the RI.
Cubby’s condition continued to deteriorate and he was euthanized early on day 2 and submitted for necropsy. Multiple tissues contained petechial hemorrhages. The bone marrow was highly cellular and contained a monomorphic population of round cells with multiple features of malignancy. Only rare normal hemopoietic cells were seen. Additional cytochemical and histochemical stains were not done, but lymphosarcoma and lymphocytic leukemia were most likely given the associated hypercalcemia. Although FDPs were not elevated, there was clinical and histologic evidence of DIC&F, likely secondary to neoplasia and paraneoplastic processes.
Erythrocyte in which the hemoglobin is displaced to one side due to oxidative damage to the lipid membrane.
Increase in the number of neutrophils in peripheral blood.
Increase in the number of monocytes in peripheral blood.
Difference between unmeasured anion and cation concentrations, calculated using the formula: (Na+ + K+) minus (Cl- + HCO3-.)
Calcium that is not bound to proteins in serum and is biologically active.
Break-down product of hemoglobin.
Concurrent decreased concentration of albumin and globulins.
Process of obtaining thoracic fluid for cytologic evaluation.
Fluid accumulation comprising peripheral blood; resembles peripheral blood but lacks platelets if more than a few hours old. Erythrophagia by macrophages is also present.
Volume of erythrocytes per liter of whole blood. Reported as L/L (calculated: MCV x RBC count). Equivalent to PCV (%) determined by centrifugation of blood in a microhematocrit tube
Term to describe the milky appearance of plasma.
Nonspecific term for sublethal or lethal injury to hepatocytes due to various causes, e.g. hypoxia, toxins, infection.
Activated clotting time; cage-side diagnostic test used to evaluate the intrinsic and common coagulation pathways.
Anucleate (in mammalian species), immature erythrocyte containing cytoplasmic RNA and ribosomes which are precipitated by staining with new methylene blue.
Reticulocyte production index; a calculated value designed to determine if the regenerative response is adequate for the degree of anemia. Corrects for the longer life of a young reticulocyte and the relative increase in reticulocytes in the presence of a low hematocrit (anemia). Reported for dogs only.
Average erythrocyte size in femtoliters (measured or calculated PCV or Hct÷RBC).
Replacement of hemopoietic tissue by abnormal tissue such as neoplastic cells, fibrosis, or granulomas,and often resulting in cytopenia(s) of normal hemopoietic cell lines.
Erythrocyte with even projections all around its membrane; often an artifact but can be a pathologic change. Echinocytes are classified as types 1 and 3 depending on the length and sharpness of the projections (spicules).
Increases serum urea and/or creatinine.
Referring to lymphocytes and tissues where lymphocytes develop.
Increase in free calcium that may accompany certain neoplasms, often due to tumor cell production of parathyroid hormone-related protein (PTHrP)
Impaired bile flow.
General term for fat, including triglycerides, phospholipids, cholesterol.
Release of less mature neutrophil stages (bands, metamyelocytes, myelocytes) from the marrow into the peripheral blood in response to inflammation.
Solid malignant lymphoid tumor.
