
Case Studies
Case 1. Micky
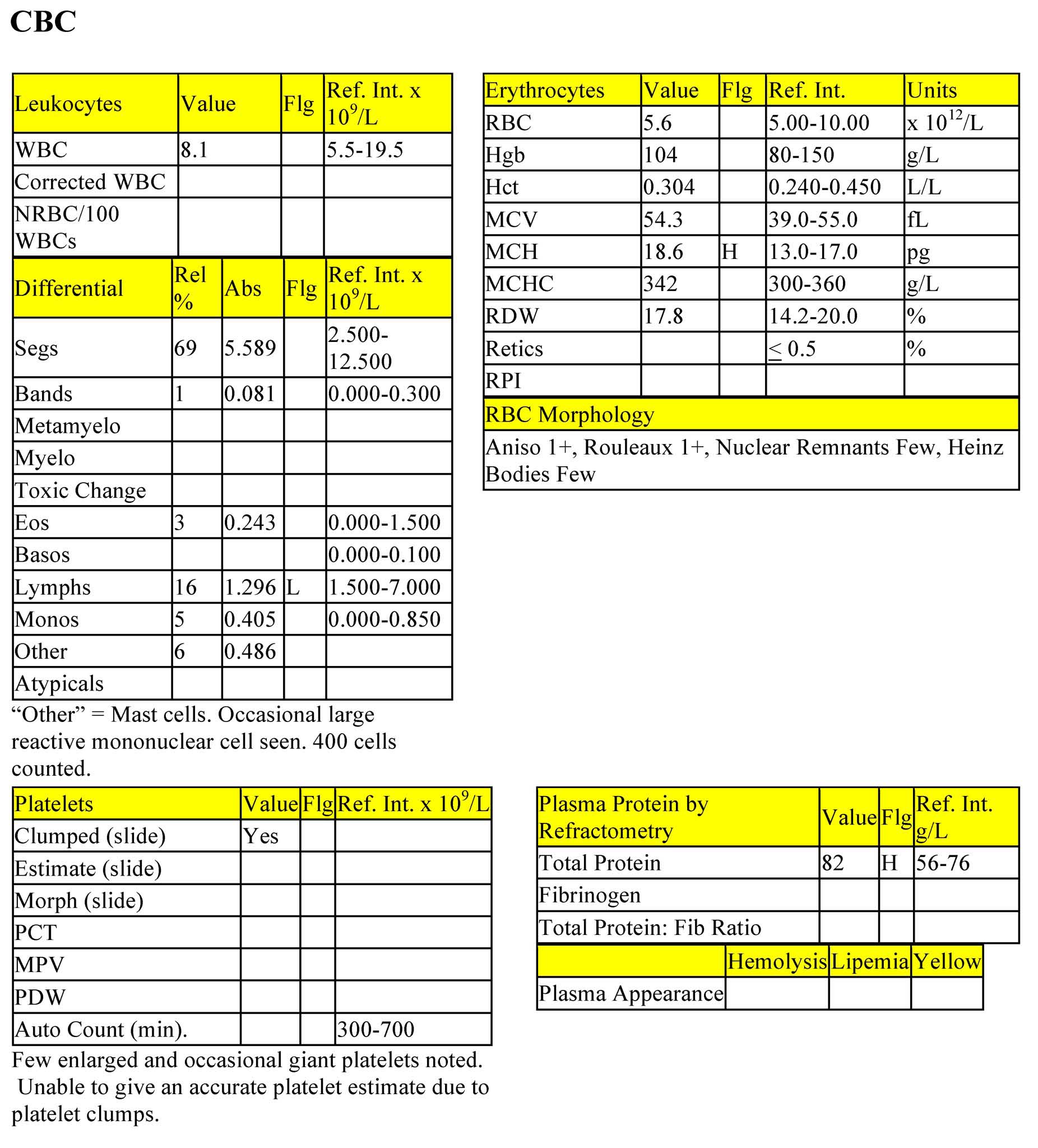
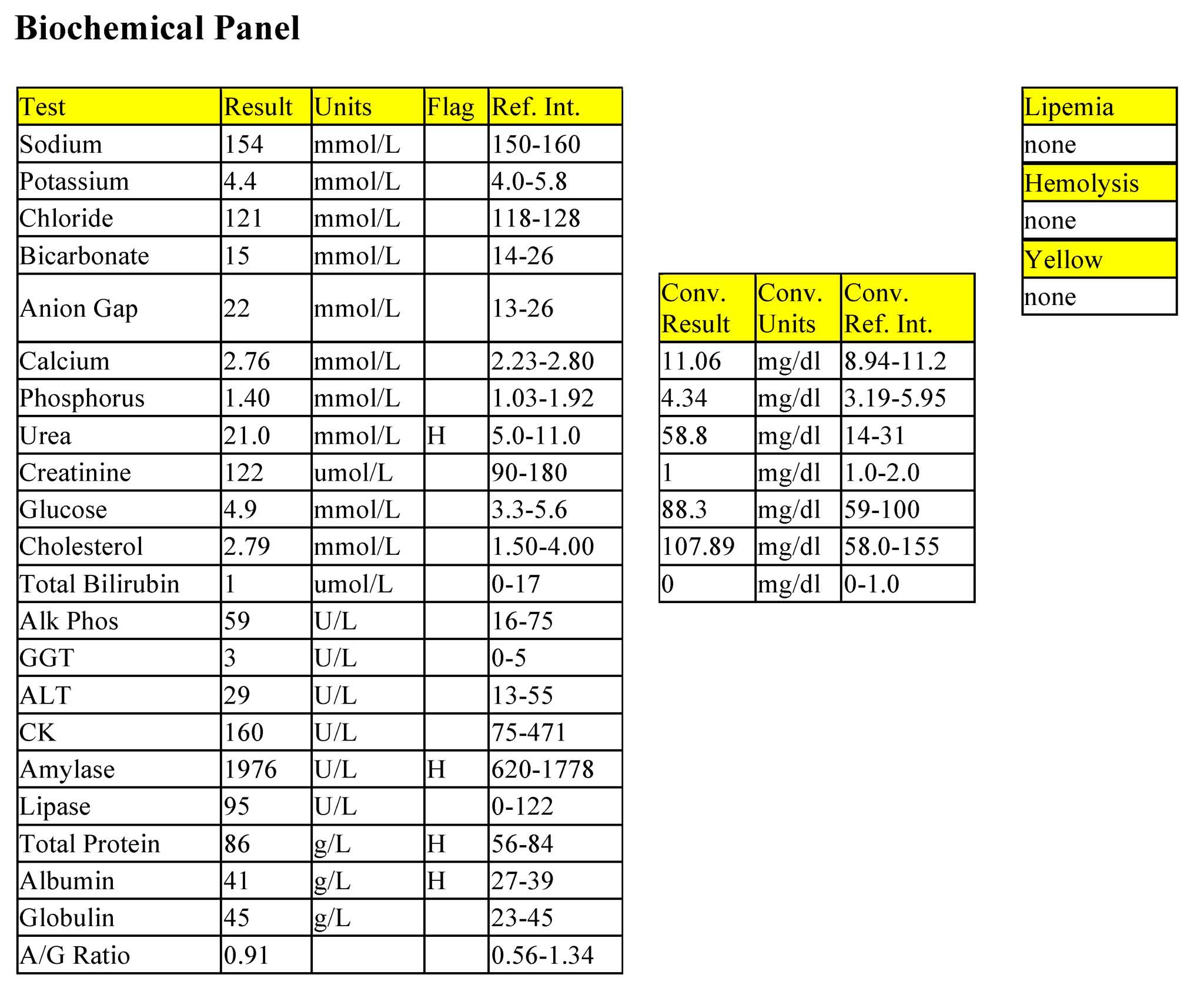
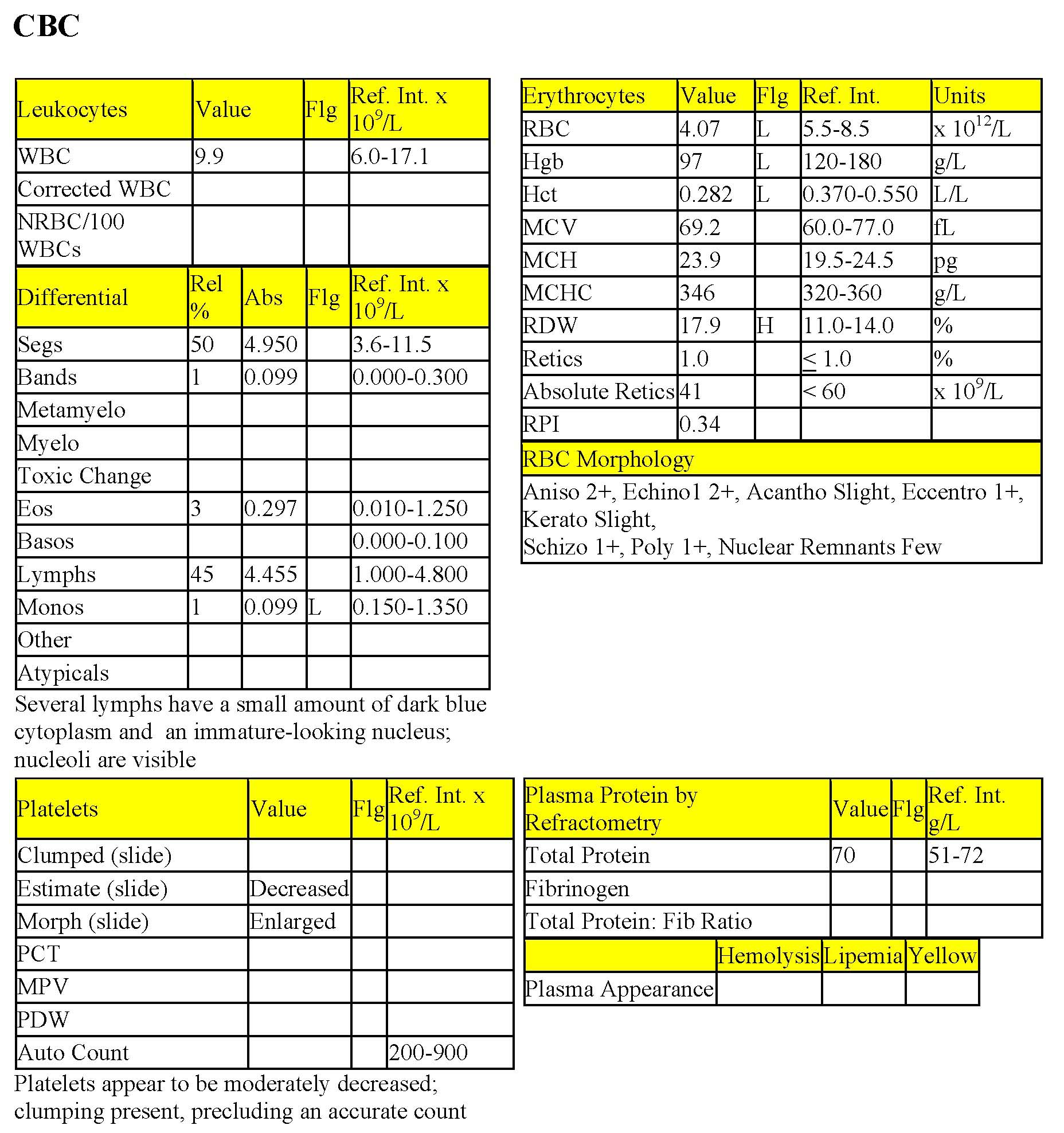
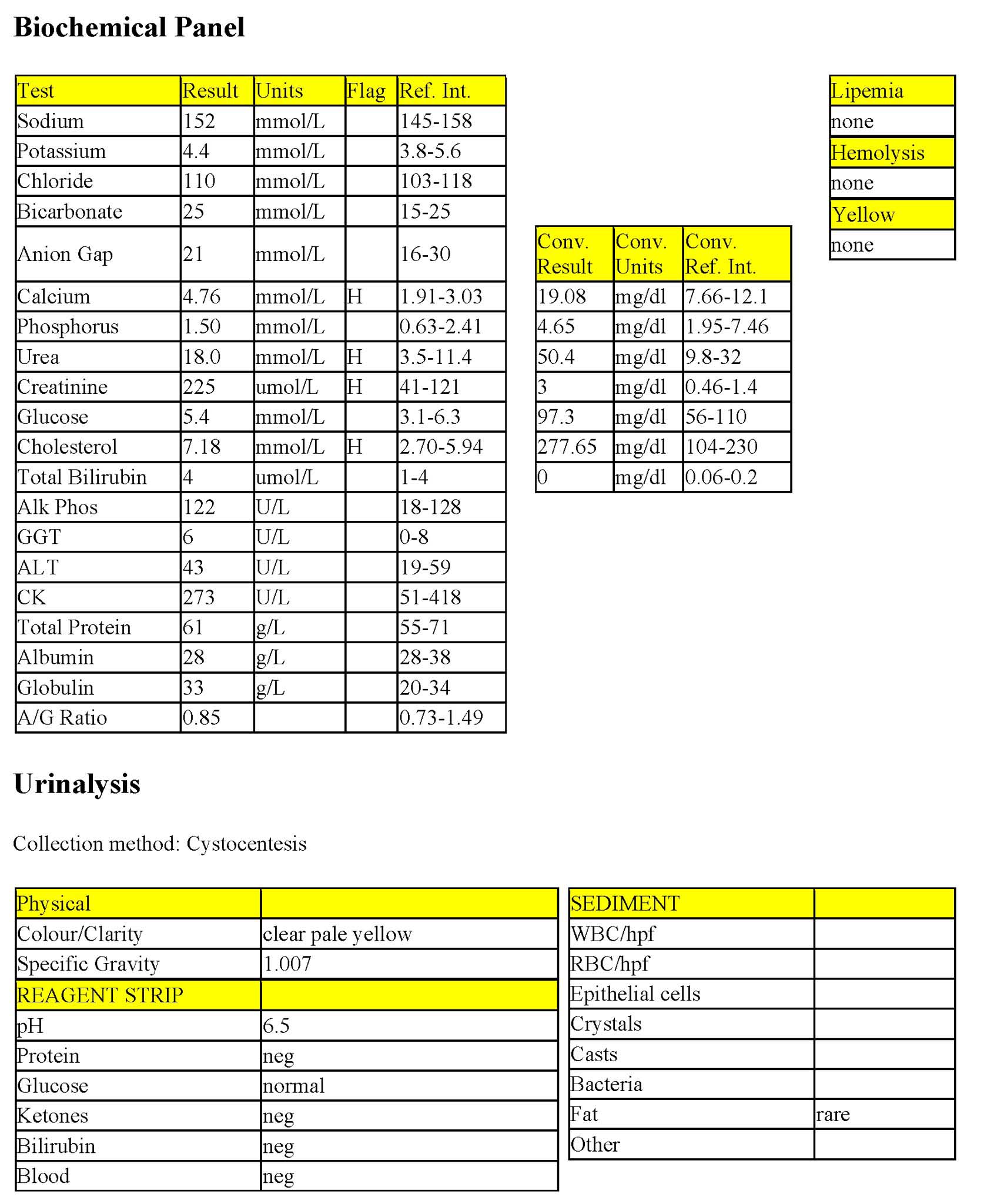
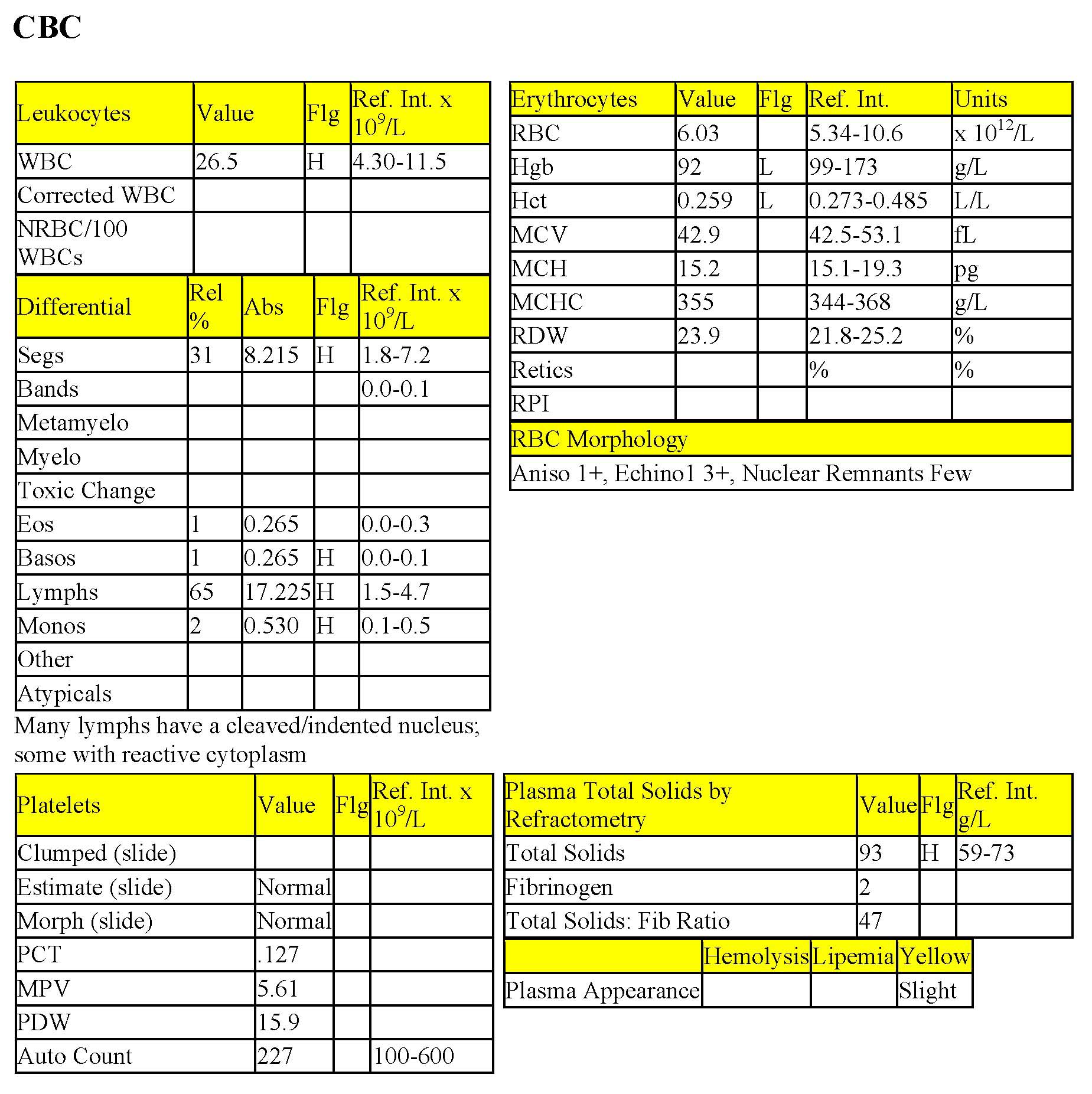
Micky, a 17-year-old M(c) Siamese cat, had recurrent diarrhea (containing blood and mucus) for 5 months.
CBC
The erythrogram is unremarkable. The mild increase in MCH is not considered to be clinically significant. Cats can have rouleaux of up to 1+. Few nuclear remnants and Heinz bodies are commonly seen in cats due to their nonsinudoidal spleens and the increased sensitivity of their hemoglobin to Heinz body formation, respectively. The leukogram is unremarkable with the exception of the mild lymphopenia consistent with the stress of illness and the presence of mast cells (Fig. 3.12). Mastocytemia can occur with certain inflammatory processes or with mast cell neoplasia. Neoplastic mastocytemia can occur as a progression of visceral or cutaneous mast cell tumors as well as a primary bone marrow-derived mast cell leukemia. There is a mild increase in total solids, suggesting dehydration.
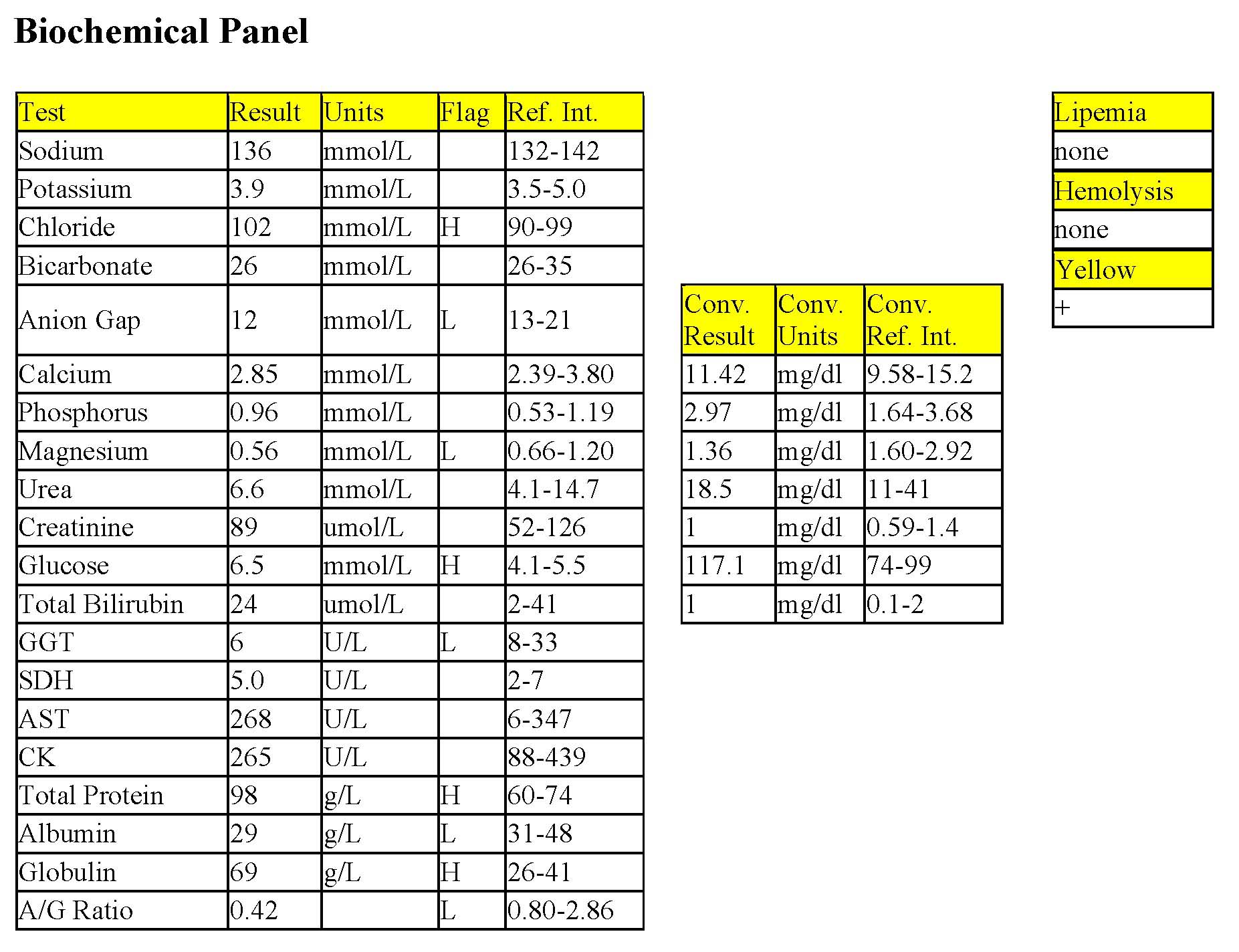
Biochemical Panel
The increased urea without a corresponding increase in creatinine could be due to intestinal hemorrhage rather than poor renal perfusion or renal disease. A urinalysis would be required to assess urine concentrating ability. Given the presence of blood in the stool, increased urea synthesis from the rich amino acid source (blood) in the intestinal tract, is likely. The mild increase in amylase activity may relate to intestinal pathology. Mild panhyperproteinemia supports dehydration.
- The history and presence of mast cells in the peripheral blood suggest mast cell neoplasia in this case. Imaging studies of Micky’s abdomen were done and the spleen and liver were found to be enlarged. Fine needle aspirates of these two organs revealed large numbers of well-differentiated mast cells. A diagnosis of systemic mast cell neoplasia, including leukemia, was made and Micky was euthanized. Histamine release from the malignant mast cell population stimulates gastric acid secretion resulting in gastric and duodenal ulceration. Blood may be present in both feces and vomitus. The spleens of cats with this neoplasm are often greatly enlarged. Peritoneal effusion frequently occurs and may also contain mast cells. Abdominocentesis can be a quick, minimally invasive diagnostic procedure in these cases.
Case 2. Katie
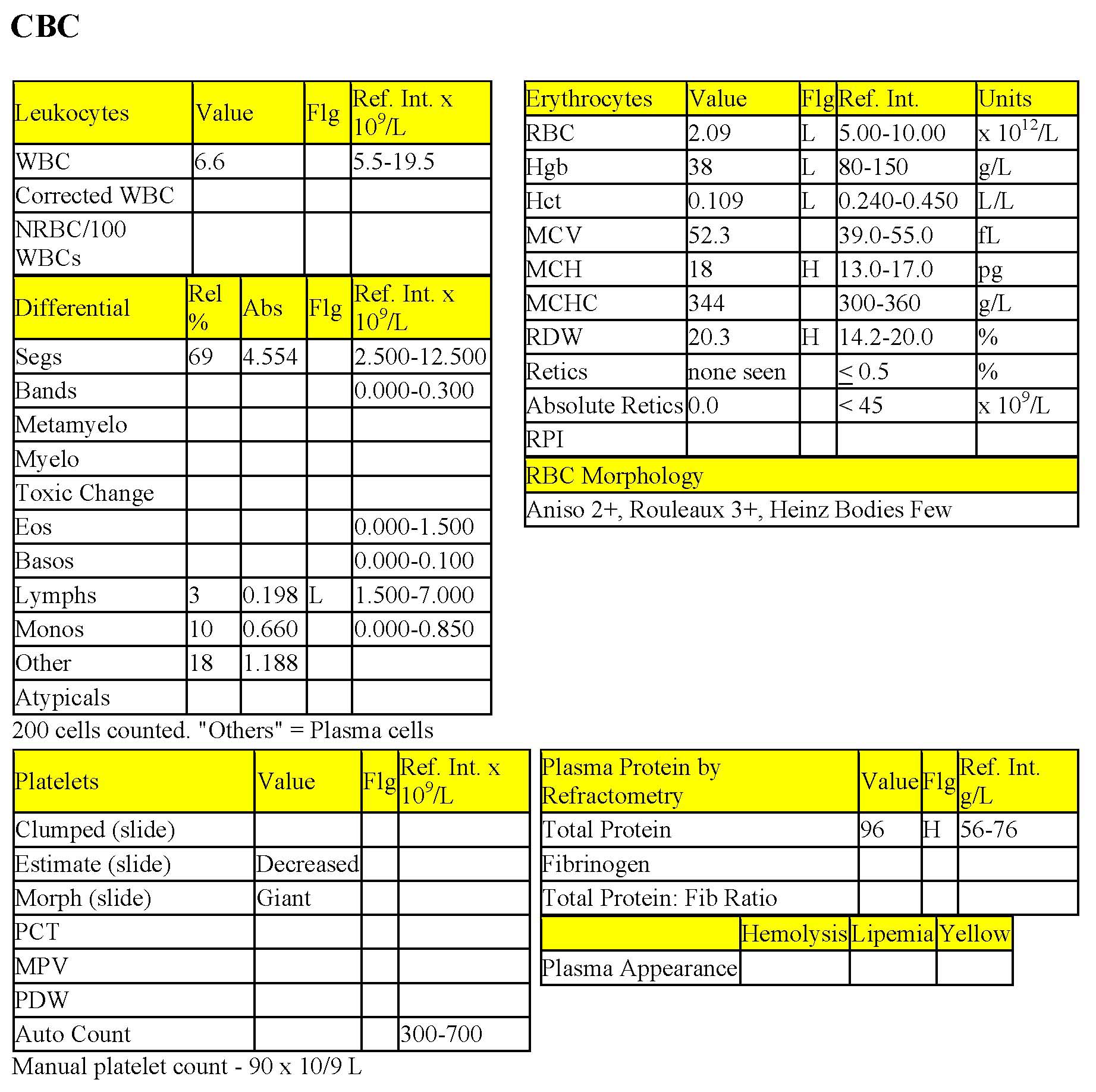
Katie, a 10-year-old F(s) DSH cat had weight loss for several months and anorexia for a few days prior to admission. Physical examination revealed a palpable mass in the cranial abdomen, which was determined to be an enlarged liver on radiographs.
CBC
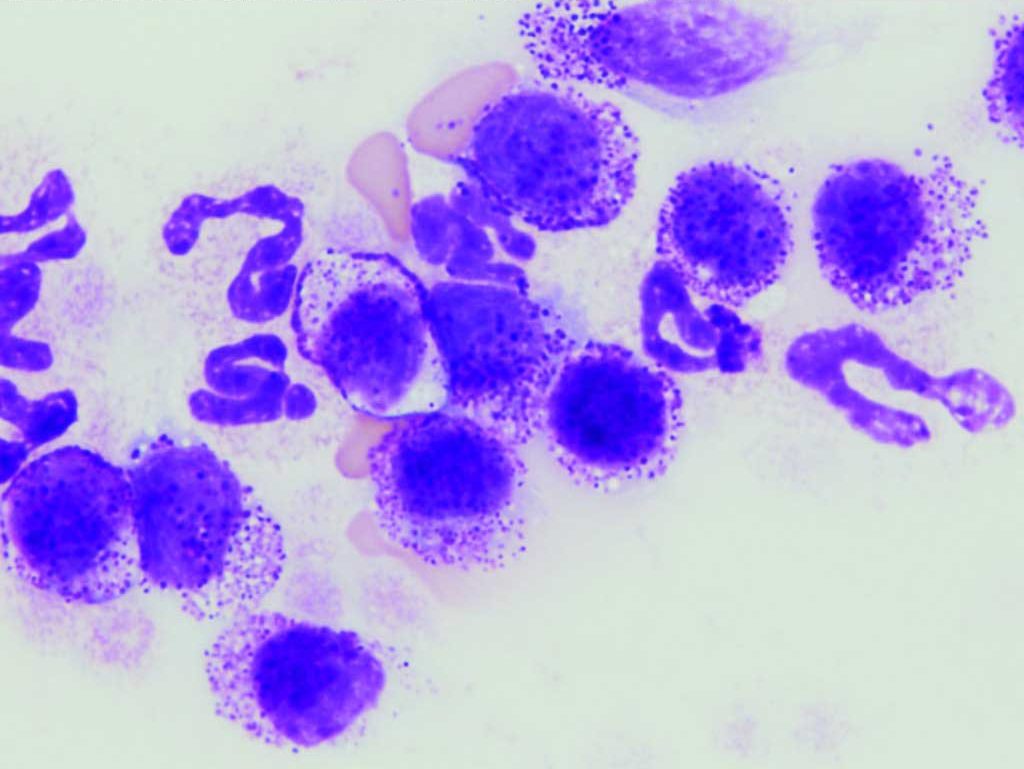
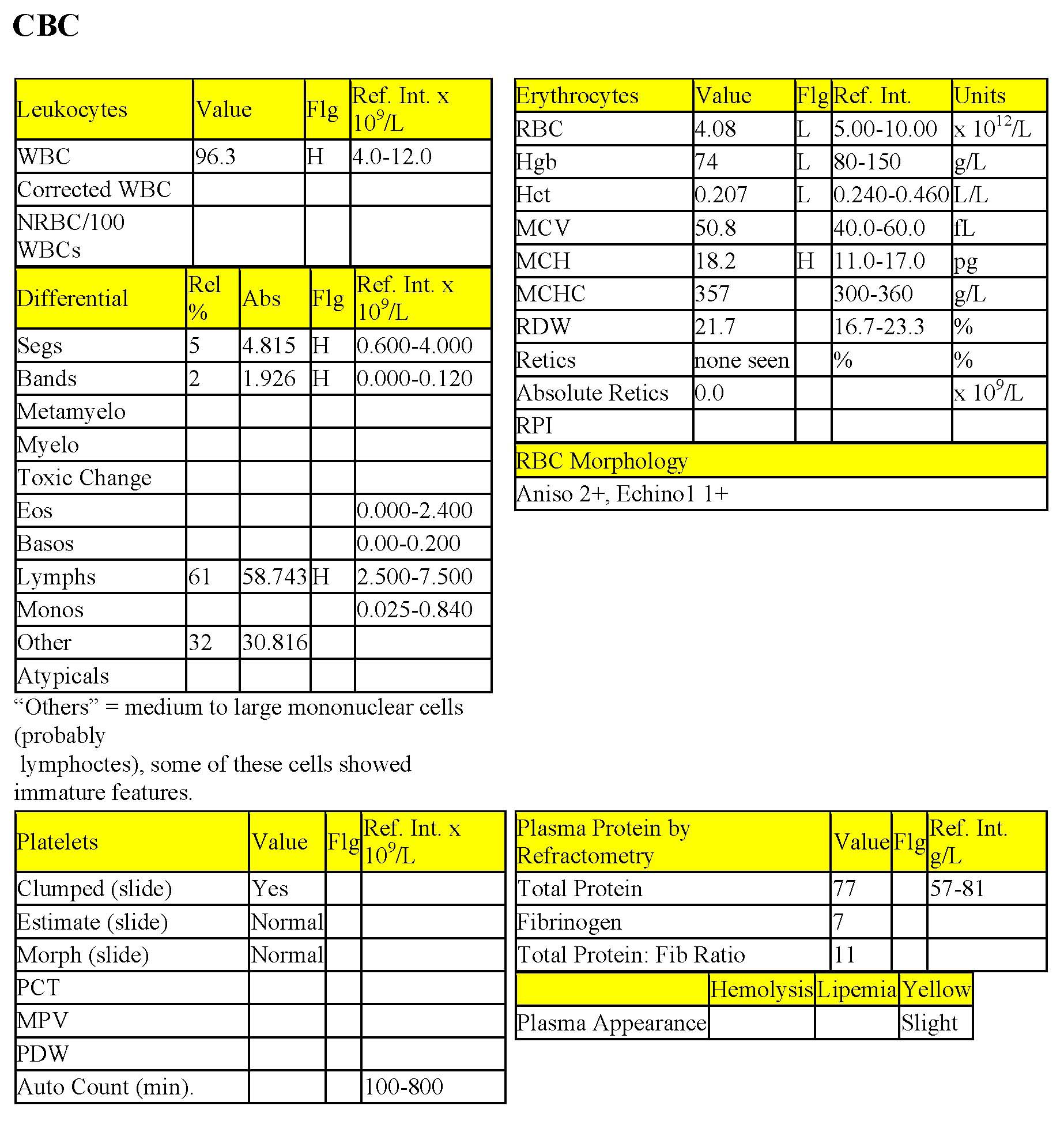
Katie has a severe nonregenerative anemia. Mild increases in MCH and RDW are not considered to be significant. The rouleaux formation noted on smear evaluation is excessive and may relate to the hyperproteinemia detected by refractometry. The leukogram is within RI with the exception of the severe lymphopenia, likely due to the stress of illness. Also, there are high numbers of plasma cells detected on the leukocyte differential count that suggest plasma cell leukemia. The presence of malignant plasma cells in the bone marrow could be responsible for the nonregenerative anemia and moderate thrombocytopenia.
Biochemical Panel
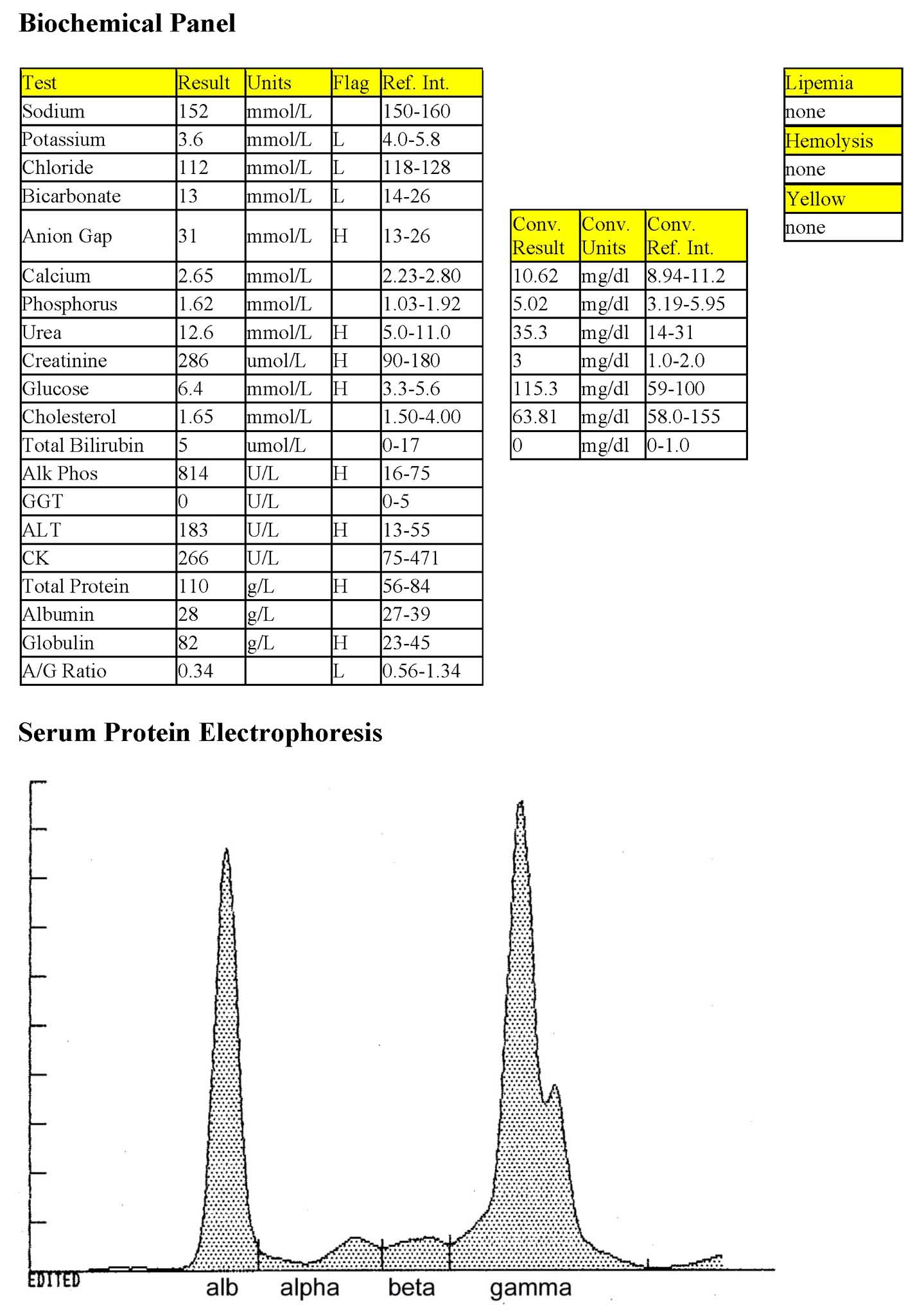
Mild hypokalemia may be due to lack of intake or increased losses. Vomiting, though not noted in the history, could result in mild hypochloremia. The high anion gap metabolic acidosis may relate to poor tissue perfusion, lactic acidosis, and renal acid retention. Mild azotemia must be interpreted in relation to USG. Very mild hyperglycemia is likely due to stress as postprandial sampling is ruled out in this case. The marked elevation in ALP activity and mild increase in ALT activity indicate hepatobiliary pathology consisting of both cholestasis and hepatocellular damage. There is a marked hyperproteinemia and low A/G ratio which is due to hyperglobulinemia.
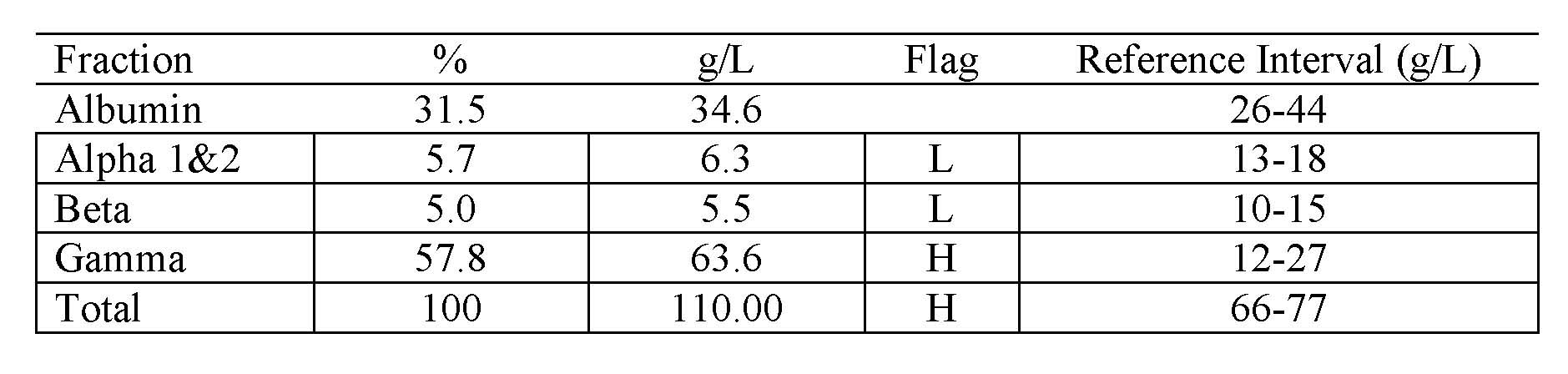
Serum Protein Electrophoresis and Radial Immunodiffusion
Alpha- and beta globulins are decreased and gamma globulins are markedly increased. The electrophoretogram shows a narrow-based spike with a small “shoulder” in the gamma region. Radial immunodiffusion revealed very high levels of IgA protein.
Bone Marrow
Bone marrow aspirates were highly cellular. Plasma cells were increased in all smears and dominated the cell population in many smears. Maturation of erythrocytes was impaired. Granulopoiesis was reduced. Megakaryocyte numbers were decreased and nuclei were immature relative to their cytoplasm.
- Katie was diagnosed with plasma cell sarcoma involving the bone marrow and manifesting as plasma cell leukemia. Hepatic involvement was also likely. The IgA monoclonal gammopathy resulted in hyperproteinemia and hyperviscosity. Hyperviscosity leads to poor tissue perfusion and, sometimes, platelet dysfunction (not seen in this case). The intense rouleaux seen on blood smear evaluation resulted from the hyperproteinemia. Neoplastic plasma cells in the bone marrow had affected normal hemopoiesis causing bicytopenia. Urine was not available to determine concentrating ability and also to evaluate by urine electrophoresis for the presence of Bence Jones proteinuria. Katie was in pain and was euthanized immediately after bone marrow was obtained.
Case 3. Betty
Betty, a 3-year-old Holstein-Friesian cow, had severe udder edema, enlarged inguinal and prefemoral lymph nodes, and diarrhea.
CBC
There is a mild nonregenerative anemia with unremarkable RBC morphology. The mildly increased MCH is unlikely to be clinically significant. The marked leukocytosis is characterized by a mild neutrophilia with a moderate left shift, and severe lymphocytosis. Leukocytes in the “other” category are probably also lymphocytes, but with more atypia. Features of these cells include: prominent, large, multiple nucleoli; mitotic figures; and binucleation. Total solids to fibrinogen ratio is in the “grey zone” that could indicate absolute hyperfibrinogenemia, dehydration, or both.
Biochemical Panel
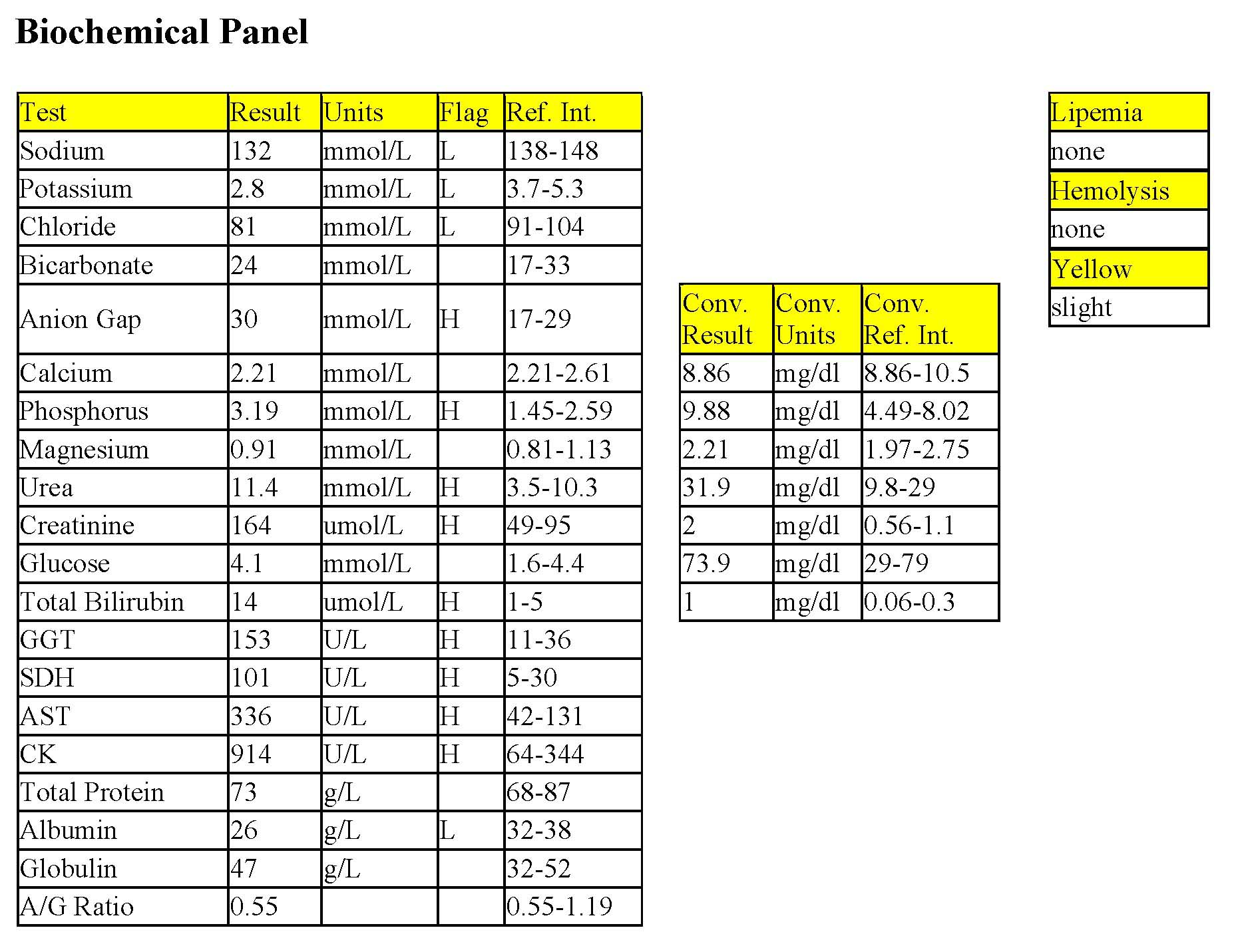
Sodium, potassium, and chloride are all decreased suggesting decreased intake, possibly coupled with increased losses through the intestinal tract, renal system, or both. Chloride is also low relative to sodium which may be due to pooling of HCl in the abomasum. The bicarbonate is within reference limits, but anion gap is slightly elevated; these changes can occur with a mixed acid-base disturbance. Metabolic alkalosis from abomasal stasis together with metabolic acidosis from lactic acid accumulation, renal acid retention, or both, is possible. Phosphorus, urea, and creatinine elevations indicate azotemia. Urinalysis is required to assess urine concentrating ability. Mild hyperbilirubinemia and moderately increased GGT activity suggest cholestasis. Moderately increased SDH activity indicates concurrent hepatocellular leakage. Mild increases in CK and AST activities are consistent with muscle injury. Alternatively, AST could be, at least in part, from the liver. Albumin is low and the albumin to globulin ratio is low normal. Hypoalbuminemia can occur with inflammation, decreased protein intake, or increased losses e.g. through the intestinal tract given the history of diarrhea. Given the left shift, albumin synthesis could be reduced through its role as a negative acute phase protein.
- Betty had lymphocytic leukemia or a leukemic profile related to solid tissue LSA. Nonregenerative anemia is likely secondary to the presence of neoplasia in the bone marrow. The left shift could be due to an unidentified inflammatory process or disorderly granulopoiesis related to tumor within the bone marrow. Enlarged lymph nodes suggest their involvement in the neoplastic process as well. Bone marrow and lymph node examination would have been useful in Betty’s case, but these were not done. A BLV test to detect antibody against the virus was negative. This finding suggests that Betty had sporadic, rather than enzootic, lymphosarcoma. At 3 years, Betty would have been rather young to have BLV-related neoplasia. However, the BLV AGID test was used rather than the ELISA which is more sensitive since it detects antibodies in addition to anti-gp 51. Therefore, BLV cannot be completely ruled out as a cause of neoplastic disease in this case.
Case 4. Prince
Prince, a 1-year-old M Golden Retriever dog, was referred with suspected renal failure. The dog was lethargic but alert upon arrival.
CBC
Prince has a moderate nonregenerative anemia. Despite the polychromasia noted on smear examination, reticulocytes (% and absolute count) and RPI are not increased. Red cell pathology is present: slight acanthocytes may be incidental in this case; eccentrocytes suggest oxidant injury, however a regenerative response would be expected if this were the primary problem; keratocytes and schizocytes may indicate fibrin strand injury which can occur with DIC&F. Despite the illness, Prince is not lymphopenic and several lymphocytes are darkly stained, immature, and contain nucleoli (Fig. 3.13). Moderate thrombocytopenia is also present. Bicytopenia and lymphocyte atypia suggest possible lymphoid neoplasia with secondary effects on normal hemopoiesis.

Biochemical Panel
Prince has a marked hypercalcemia. Although there are several possible etiologies for hypercalcemia, malignancy (parathyroid hormone-related protein [pb_glossary id="3520"]PTHrP[/pb_glossary] production by neoplastic cells) is likely in this case. Mild azotemia in the presence of near isosthenuria (urine SG 1.007) indicates renal disease, which is probably secondary to hypercalcemia. Mild hypercholesterolemia could be due to postprandial sampling as there was no indication that this was collected after fasting or from an anorexic patient.
Urinalysis
The only significant finding on urinalysis is the SG of 1.007, which is near isosthenuria, and inappropriate given the azotemia. Hypercalcemia antagonizes the activity of antidiuretic hormone in the kidneys. Hypercalcemia can also cause renal tubular damage leading to renal disease.
- Although bone marrow examination was indicated, lymph nodes were found to be enlarged and these were aspirated as an alternative to the more invasive bone marrow procedure. Lymph node cytology confirmed the presence of LSA. The presence of circulating neoplastic lymphocytes indicates a concurrent leukemic profile, even though numbers are not high. Bone marrow occupation with neoplastic lymphocytes would explain the anemia and thrombocytopenia. To assess the possibility of DIC&F, prothrombin time (PT), partial thromboplastin time (PTT) and fibrin/fibrinogen degradation products (FDP) were measured, and these were within RI. Chemotherapy and fluid therapy were instituted. The hypercalcemia resolved and Prince was returned to the care of the referring veterinarian. CBCs would have to be done regularly, both to avoid chemotherapeutic suppression of normal bone marrow activity, and to monitor the existing bicytopenia. No other follow-up is available.
Case 5. Nickle
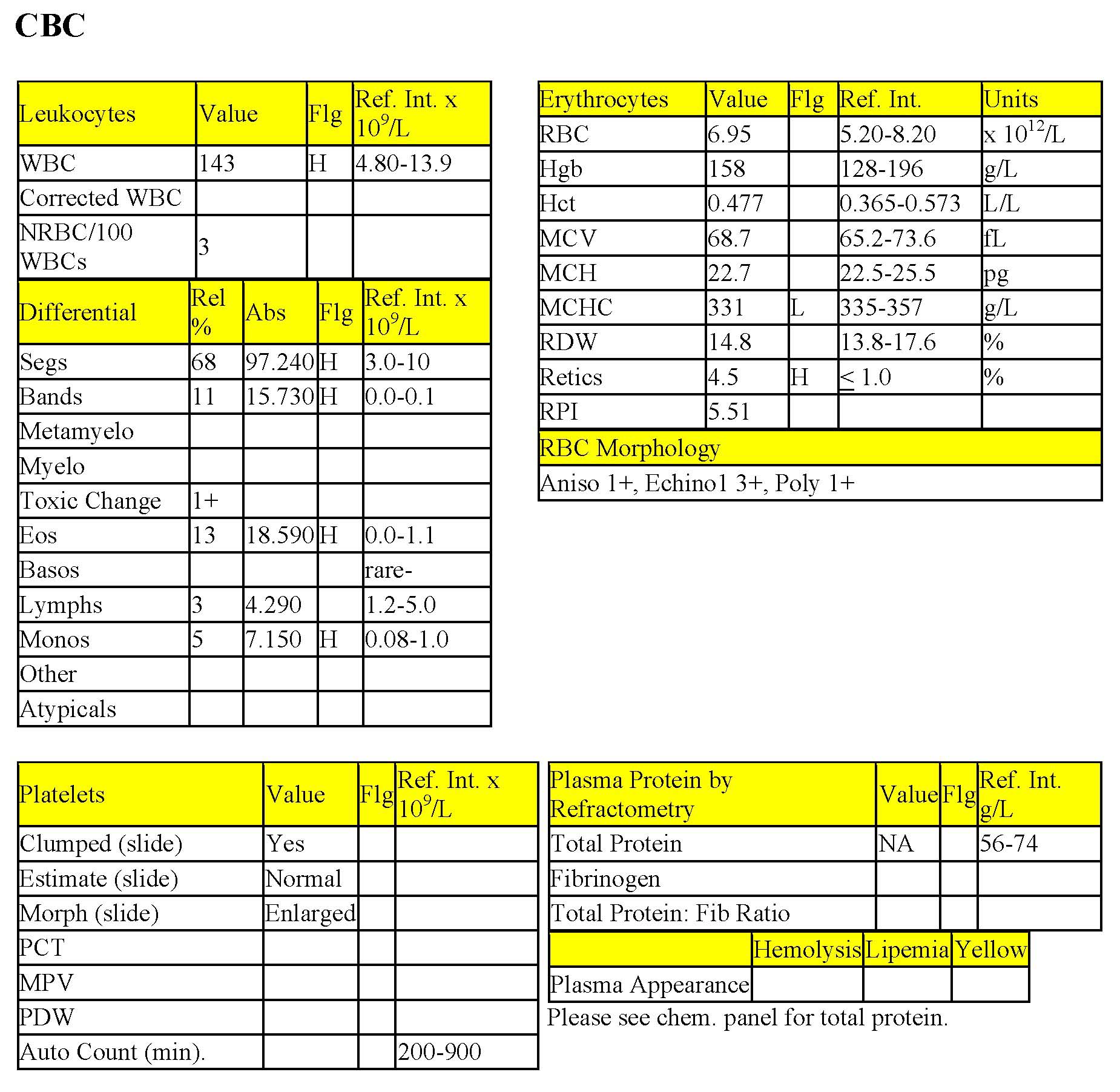
Nickle, a 10-year-old M(c) American Spaniel dog, had lethargy and anorexia for 3 days. Nickle has a fever and possible splenic mass.
CBC
Although anemia is not present, there is a regenerative response (increased reticulocytes, both % and absolute count, RPI, and polychromasia). The Hct may be low for this particular dog. Alternatively, hypoxia may be present; arterial pO2 would help determine if the regenerative response is due to tissue hypoxia. Other considerations are recovery from prior anemia or ongoing low grade hemolysis or blood loss. The severe leukocytosis is characterized by severe neutrophilia, a severe left shift with mild toxic change, marked eosinophilia, and moderate monocytosis. There is a lack of stress lymphopenia. Smear evaluation revealed atypical blast cells which had features of both granulocytes and monocytes. There were also nucleated RBCs with abnormal features including clover-leafed nuclei and occasional mitoses.
Biochemical Panel
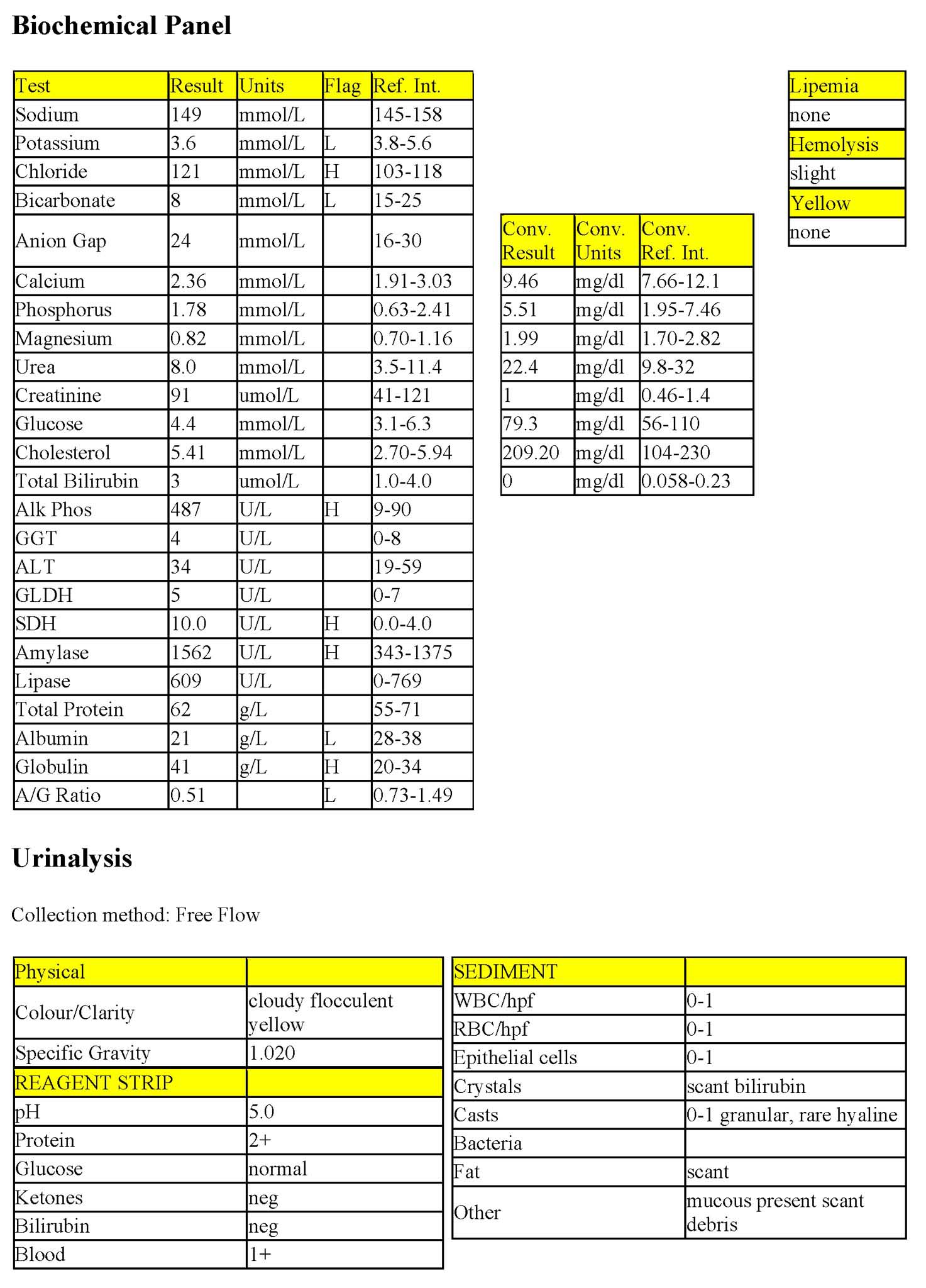
Mild hypokalemia may be due to anorexia or increased losses. Hyperchloremic metabolic acidosis is consistent with renal or intestinal bicarbonate loss. Amylase activity is mildly increased and could be pancreatic or intestinal in origin. Mildly increased ALP activity may be the steroid isoform or biliary tract origin in this case. Although ALT and GLDH activities are not increased, hepatocellular injury is indicated by the mildly increased SDH activity. Hypoalbuminemia may be due to proteinuria in this case. Mild hyperglobulinemia could be further characterized with serum protein electrophoresis.
Urinalysis
Proteinuria may be significant and could be confirmed by measuring UPC ratio. Granular casts suggest tubular injury; hyaline casts could relate to proteinuria.
- There was a strong suspicion of bone marrow neoplasia, possibly myelomonocytic leukemia, in this case. The suspected splenic mass could be due to occupation of the spleen by neoplastic cells. Renal involvement is also possible. Bone marrow examination, along with cytochemistry, immunohistochemistry, and potentially, molecular studies, may be required to determine neoplastic cell lineage. If malignancy were at an early precursor level, eosinophils and erythrocytes could also be involved. Alternatively, neutrophilia and eosinophilia can occur as paraneoplastic processes if the malignant population is elaborating certain growth factors or cytokines, and dysplastic changes can occur in “normal” cell lines (such as erythroid cells) due to the deranged bone marrow microenvironment and function. Nickle’s condition deteriorated rapidly, he began vomiting blood, and, because of the grave prognosis, he was euthanized. Unfortunately, a necropsy was not done.
Case 6. Feather
Feather, a 6-year-old Clydesdale mare, had bilateral periorbital swelling for a few days.
CBC
The mild anemia cannot be characterized as regenerative or nonregenerative given the lack of reticulocyte release in this species. However, the MCV is low normal and the RDW is within the RI suggesting that large (immature) cells are not present. There is a severe leukocytosis that is mainly due to lymphocytosis. The mild neutrophilia and monocytosis may be due to mild inflammation; however, a stress response could also be considered. Lymphocyte numbers should be affected by stress unless there is an overriding reason for lymphocytes to be within the RI or increased. The lymphocyte cytoplasm appears reactive (stained dark blue) possibly from antigenic stimulation or due to neoplasia. Abnormal lymphocyte nuclear morphology is reported, also suggestive of possible neoplasia. The hyperproteinemia is discussed in the biochemistry section. There is no hyperfibrinogenemia as might be expected if inflammation were present.
Biochemical Panel
Mildly decreased anion gap may relate to the hypoalbuminemia (decreased “unmeasured” anion). The other changes are mild and unlikely to be of clinical significance with the exception of the protein profile. Moderate hyperproteinemia is due to moderate hyperglobulinemia. Serum protein electrophoresis demonstrated a monoclonal peak in the gamma globulin fraction. Radial immunodiffusion revealed IgG gammopathy consistent with paraprotein production by B lymphocyte or plasma cell neoplasia. Fine needle aspirates of periorbital swellings contained lymphocytes similar to those in the peripheral blood. Mitotic figures were frequent.
Feather was euthanized and disseminated LSA was confirmed. Immunohistochemistry indicated that the neoplastic cells were B lymphocytes. Non-neoplastic T lymphocytes infiltrated the neoplastic population. Although the B cells had not differentiated to plasma cells, they were producing immunoglobulin similar to that in case 2 (Katie).
All tests on the complete blood count (CBC) that evaluate erythrocytes, including morphologic examination on the peripheral blood smear.
Average amount of hemoglobin per erythrocyte (calculated: hemoglobin÷RBC count).
Piece of the nucleus that persists in the mature erythrocyte. May be seen in healthy animals, especially cats, and those with regenerative anemias, or hypofunctioning spleens.
Oxygen-carrying molecule within erythrocytes.
Aggregate of denatured hemoglobin within a RBC, caused by oxidative damage.
Constellation of: retention of metabolic waste products, acid-base and electrolyte disturbances, and compromised urine concentrating ability that develops when the functional mass of the kidneys is reduced by 70% or more; may be acute or chronic.
Technique used to obtain samples for cytologic evaluation, using suction.
Process of obtaining abdominal fluid for cytologic evaluation.
Method of measuring the protein content of a fluid that relies on refraction of light, which is proportional to the quantity of solids in solution.
Difference between unmeasured anion and cation concentrations, calculated using the formula: (Na+ + K+) minus (Cl- + HCO3-.)
Process that adds acid (H+) to the blood or removes base (HCO3-); blood pH may or may not be decreased.
Increases serum urea and/or creatinine.
Impaired bile flow.
Technique combining protein electrophoresis and immunodiffusion to identify different immunoglobulin classes (e.g. IgA, IgG).
Part of hemopoiesis dealing with the production of granulocytes from stem cells to mature circulating neutrophils, eosinophils, and basophils.
Increase in the number of neutrophils in peripheral blood.
Release of less mature neutrophil stages (bands, metamyelocytes, myelocytes) from the marrow into the peripheral blood in response to inflammation.
Process that adds base (HCO3-) to the blood or removes acid (H+); blood pH may or may not be increased.
Most abundant plasma protein in health; maintains oncotic pressure.
Anucleate (in mammalian species), immature erythrocyte containing cytoplasmic RNA and ribosomes which are precipitated by staining with new methylene blue.
Erythrocyte with little central pallor and several irregular membrane projections.
Erythrocyte in which the hemoglobin is displaced to one side due to oxidative damage to the lipid membrane.
Crescent-shaped cells that are formed from mechanical shearing (usually due to fibrin strand deposition) of the red cell.
An erythrocyte fragment created by shearing trauma to erythrocytes within the vascular system; often the fragment which has been sheared off to form a keratocyte.
The end product of coagulation, produced by the conversion of fibrinogen.
PTH; hormone that increases serum calcium levels.
Urine specific gravity between 1.008 and 1.012, reflecting urine that has been neither diluted nor concentrated by the kidneys.
Prothrombin time; diagnostic test used to evaluate the extrinsic and common pathways.
Partial thromboplastin time; diagnostic test used to evaluate the intrinsic and common pathways.
Fibrin/fibrinogen Degradation Products; increased concentration of these products supports a diagnosis of DIC&F.
Reticulocyte production index; a calculated value designed to determine if the regenerative response is adequate for the degree of anemia. Corrects for the longer life of a young reticulocyte and the relative increase in reticulocytes in the presence of a low hematocrit (anemia). Reported for dogs only.
Erythrocyte rupture or destruction; may occur in vitro or in vivo as a pathologic process.
Cytoplasmic abnormalities seen in neutrophils that have not matured normally in the bone marrow. Abnormalities include retention of primary granules, vacuolation, darker staining due to retention of ribosomes, and deposits of rough endoplasmic reticulum (Döhle bodies).
Increase in the number of eosinophils in peripheral blood.
Increase in the number of monocytes in peripheral blood.
Nonspecific term for sublethal or lethal injury to hepatocytes due to various causes, e.g. hypoxia, toxins, infection.
